After a Congressional investigation the lying spokesman for the US drug industry on vaccine safety Dr. Paul Offit, of the Childrens’ Hospital of Philadephia, was named in a formal Congressional report for voting himself rich as a member of the US Advisory Committee on Immunization Practices (ACIP). Crooked Offit voted for his own patented vaccine Rotavirus to be introduced into the US childrens’ vaccine schedule when he was meant to be looking out for the health and safety of US children. [So no change there then]. Offit has made millions of dollars from the patent for the vaccine which he held in partnership with vaccine maker Merck.
And governments pretend they do not understand when the public do not believe them. And they still keep appointing some crooked “experts” like this to their oversight panels.
Offit has already been caught lying publicly twice about vaccine safety issues – see CHS article here: Paul Offit – “Doctor of Vaccine Profit” Caught Lying – Again – Orange County Register
He has also claimed children can withstand 100,000 vaccines administered at once when the US government has paid out a settlement of US$20m to Hannah Poling who developed an autistic condition caused by receiving 9 vaccines in one day: US Government In US$20 million Legal Settlement For Vaccine Caused Autism Case
The full text of the Congressional investigation report is set out at the end of this article.
It shows Offit voted “yes” three times for including Rotavirus vaccine on the US childhood vaccine schedule and abstained only once for a vote to rescind the recommendation of Wyeth’s vaccine after it had been found to cause adverse events. Dr. Offit began his tenure on ACIP in October of 1998.
The Report shows Dr. Offit:-
- had already been awarded the patent on the Rotavirus vaccine which he shares in development with Merck
- received a $350,000 grant from Merck for Rotavirus vaccine development
- acts as a consultant to Merck.
- out of four votes pertaining to the ACIP’s rotavirus statement, he voted yes three times, including voting for the inclusion of the rotavirus vaccine in the VFC program.
- Dr. Offit abstained from voting on the ACIP’s rescission of the recommendation of the Wyeth rotavirus vaccine for routine use when serious adverse reactions were being reported. He stated at the meeting, “I’m not conflicted with Wyeth, but because I consult with Merck on the development of rotavirus vaccine, I would still prefer to abstain because it creates a perception of conflict.″
The Report mentions Offit by name several times:
C. Problems Identified During the Committee’s Investigation
The Committee staff’s review of the ACIP’s consideration of the rotavirus vaccine identified serious weaknesses in the CDC’s policing of conflicts of interest on this advisory committee. On June 25, 1998, the ACIP voted to recommend the rotavirus vaccine for routine use in infants. In reviewing the minutes of ACIP meetings and the financial disclosure forms of the ACIP members, the Committee staff identified a number of troubling issues:
1. ACIP Members Do Not Fully Disclose Conflicts of Interest
Examination of ACIP members’ financial disclosure forms reveals that many members do not fill them out completely. CDC ethics officials conceded to Committee staff that they have been lax in compelling the ACIP members to provide complete and thorough information.[lxv]
………..
c. Dr. Paul Offit
Dr. Offit lists that he is a consultant to Merck on an attachment to his OGE 450, but does not disclose whether or not he received any remuneration for his services. (Exhibit 39)
And here:-
3. ACIP Members are Allowed to Vote on Vaccine Recommendations, Even When They Have Financial Ties to Drug Companies Developing Related or Similar Vaccines
……..
While ACIP members with ties to Wyeth-Lederle were not allowed to vote on recommendations for the rotavirus vaccine, those with ties to Merck and Smithkline-Beecham were allowed to vote. This stands in stark contrast to the policies of the FDA. In discussions with FDA staff on this specific issue they informed the Committee staff that when the VRBPAC is deliberating the licensure of a vaccine, a company is considered affected [an affected company is one with a direct interest] if they are direct competitors of the manufacturer of the vaccine being considered. They further clarified that that this policy was in place because of the competing interest of the affected company and not because of concerns about the release of proprietary information. Moreover, if a VRBPAC member has a direct interest with a competing firm they are automatically disqualified from participation.
At ACIP meetings from February 11, 1998, through June 17, 1999, there were eight votes related to the their approval of the rotavirus vaccine for routine use. Three of these votes were particularly notable. They include: (1) June 25, 1998 – The ACIP approved the statement recommending the rotavirus vaccine for routine use, (2) October 22, 1998 – The ACIP recommended the rotavirus vaccine be added to the Vaccines for Children Program, and (3) October 22, 1999-the ACIP rescinded its earlier decision to recommend the rotavirus vaccine.
………
b. Dr. Paul Offit (Exhibits 38-41)
Dr. Offit shares the patent on the Rotavirus vaccine in development by Merck and lists a $350,000 grant from Merck for Rotavirus vaccine development. Also, he lists that he is a consultant to Merck.
Dr. Offit began his tenure on ACIP in October of 1998. Out of four votes pertaining to the ACIP’s rotavirus statement he voted “yes” three times, including, voting for the inclusion of the rotavirus vaccine in the VFC program.
Dr. Offit abstained from voting on the ACIP’s rescission of the recommendation of the rotavirus vaccine for routine use. He stated at the meeting, “I’m not conflicted with Wyeth, but because I consult with Merck on the development of rotavirus vaccine, I would still prefer to abstain because it creates a perception of conflict.”[lxvii]
FULL TEXT OF US CONGRESSIONAL REPORT
Conflicts of Interest in Vaccine Policy Making
Majority Staff Report
Committee on Government Reform
U.S. House of Representatives
June 15, 2000
Section I
Introduction
In August 1999, the Committee on Government Reform initiated an investigation into Federal vaccine policy. Over the last six months, this investigation has focused on possible conflicts of interest on the part of Federal policy-makers. Committee staff has conducted an extensive review of financial disclosure forms and related documents, and interviewed key officials from the Department of Health and Human Services, including the Food and Drug Administration and the Centers for Disease Control and Prevention.
This staff report focuses on two influential advisory committees utilized by Federal regulators to provide expert advice on vaccine policy:
1. The FDA’s Vaccines and Related Biological Products Advisory Committee (VRBPAC); and
2. The CDC’s Advisory Committee on Immunizations Practices (ACIP).
The VRBPAC advises the FDA on the licensing of new vaccines, while the ACIP advises the CDC on guidelines to be issued to doctors and the states for the appropriate use of vaccines.
Members of the advisory committees are required to disclose any financial conflicts of interest and recuse themselves from participating in decisions in which they have an interest. The Committee’s investigation has determined that conflict of interest rules employed by the FDA and the CDC have been weak, enforcement has been lax, and committee members with substantial ties to pharmaceutical companies have been given waivers to participate in committee proceedings. Among the specific problems identified in this staff report:
§ The CDC routinely grants waivers from conflict of interest rules to every member of its advisory committee.
§ CDC Advisory Committee members who are not allowed to vote on certain recommendations due to financial conflicts of interest are allowed to participate in committee deliberations and advocate specific positions.
§ The Chairman of the CDC’s advisory committee until very recently owned 600 shares of stock in Merck, a pharmaceutical company with an active vaccine division.
§ Members of the CDC’s advisory Committee often fill out incomplete financial disclosure statements, and are not required to provide the missing information by CDC ethics officials.
§ Four out of eight CDC advisory committee members who voted to approve guidelines for the rotavirus vaccine in June 1998 had financial ties to pharmaceutical companies that were developing different versions of the vaccine.
§ 3 out of 5 FDA advisory committee members who voted to approve the rotavirus vaccine in December 1997 had financial ties to pharmaceutical companies that were developing different versions of the vaccine.
A more complete discussion of specific conflict of interest problems identified by Government Reform Committee staff can be found in Sections 4 and 5 of this report. To provide focus to the discussion, this report examines the deliberations of the two committees on one specific vaccine — the Rotavirus vaccine. Approved for use by the FDA on August 31, 1998, the Rotavirus vaccine was pulled from the market 13 months later after serious adverse reactions to the vaccine emerged. Financial disclosure forms and waivers granted to committee members who participated in these meetings were analyzed, along with their votes and actions taken during the meetings.
Section II
Laws and Regulations
Laws Governing Advisory Committees
Federal law requires that advisory committees be balanced in terms of points of view of their members and that they conduct their business in public. The law also requires that advisory committee members disclose their financial interests and recuse themselves from matters in which they have an interest. The following is a brief description of the requirements of these laws:
1. Federal Advisory Committee Act (FACA)[i]:
The FACA, signed into law by President Richard Nixon in 1972, regulates advisory committees, task forces and councils established by either the President, the federal agencies or Congress. These increasingly influential advisory bodies have been considered by many to be the A fifth branch of government.[ii] It is important to note, however, that the FACA does not address the conflict of interest of committee members; these are addressed in a separate statute and dealt with by individual agencies in the Code of Federal Regulations.[iii] The FACA’s most significant requirements fall into three basic categories:
a.) Scope of Committees: The statute clearly states that the function of advisory committees is to be Advisory only. They provide advice and recommendations that may or not may be adopted. The final determination is to be made by the official or agency involved.[iv]
b.) Requirement of Openness: The second important issue addressed by the FACA is the need for openness in the proceedings of advisory committees. With very few exceptions, all advisory committee meetings are to be open to the public and the materials distributed at the meetings, including working papers, studies agendas, etc…, are to be made available to the public for inspection.[v]
c.) Balanced Representation: Perhaps the most controversial provision of the FACA is the need for a membership that is Afairly balanced in terms of the points of view represented and the functions of the committee.[vi] The statute specifically forbids the committees to be inappropriately influenced by special interests.[vii]
2. Conflicts of Interest Statutes [viii]:
The ethics guidelines for the advisory committees are set by the agencies in accordance with federal statute, specifically 18 U.S.C. ”202-209. Under the statute, advisory committee members are considered ASpecial Government Employees (SGEs). SGEs provide temporary services to the U.S. government, not to exceed 130 days a year. As SGEs, advisory committee members must comply with Federal conflict of interest laws. 18 U.S.C. ”202-209 broadly prohibits employees, including SGEs, from participating in a decision-making process when they have a personal interest in the matters discussed, absent a waiver from the relevant parties .[ix] The types of waivers found in the statute are:
a.) (b)(1) waivers: The employee may participate when the appointing official determines that the financial interest is not substantial as to be deemed likely to affect the integrity of the services that the Government may expect.[x]
b.) (b)(2) waivers: Employee may participate if the interest is so remote or inconsequential that it will not have a special or distinct effect on the employee or his employer.[xi]
c.) (b)(3) waivers: specifically applicable to advisory committee members, this waiver will allow them to participate in matters for which he would have been disqualified, if it is determined that the need for the employees services outweigh the potential conflict of interest created by the employees financial interest.[xii] Factors that may be considered include: type of interest, identity of the person, uniqueness of the individuals qualifications, difficulty of locating a similarly qualified individual without a disqualifying interest, the dollar value of the interest- including its value relevant to the members assets, and the extent to which the financial interest will be affected by the actions of the committee.
3. Code of Federal Regulations (CFR) & Office of Government Ethics (OGE):
Since most advisory committee members are considered special government employees, the provisions in 18 U.S.C. ”201-219 that address conflicts of interest apply to them. However, the statute only provides broad guidelines, so that it is up to the individual agencies to provide the specific rules governing conflict of interest.[xiii] In the case of the Department of Health and Human Services (DHHS), these regulations can be found at 5 C.F.R. ” 2635 and in 5 C.F.R. ”2640. Under the DHHS regulations, an advisory committee member may not participate, absent a waiver, in matters in which they have a financial interest. These are divided into the following categories:
a.) Particular matter: includes matters that involve deliberation, decision, or action focused on the interests of specific persons, or a discrete and identifiable class of persons.[xiv]
b.) Particular matter involving specific parties: the code defines this term to include proceedings, applications, requests for determination, contracts, claims, controversies and/or investigations involving specific parties. The term typically involved a specific proceeding affecting the legal rights of the parties, or an isolatable transaction or related set of transactions between identified parties.[xv] This term will generally refer to the particular issue, vaccine and or company that will be directly affected by the advisory committee discussions.
c.) Particular matter of general applicability: the code defines this term as a particular matter that is focused on the interests of a discrete and identifiable class of persons, but does not involve specific parties.[xvi] This definition becomes relevant in the discussion of companies that may be indirectly affected by the proceedings of an advisory committee. In this report, the companies under this category will be referred to as affected companies.
d.) A direct and predictable effect on their financial interest: a direct effect on a financial interest is defined as a close causal link between any decision or action to be taken in the matter and any expected effect of the matter on the financial interest.[xvii] According to the CFR, the effect may actually be considered direct even though it does not occur immediately. However, the CFR also specifies that the link will not be direct in instances where the chain of causation is attenuated or is contingent upon the occurrence of events that are speculative.[xviii] On the other hand, predictable is defined in the code as a situation where there is a real possibility that the matter will be affected.
e.) Affected interests: according to the CFR, the disqualifying financial interests include: salary, indebtedness, job offer, or any other similar interests that could be affected by the matter discussed.[xix] It also includes the interests of persons other than the advisory committee members, such as a spouse, children, general partner, place of employment, organizations where the advisory committee member serves as officer, director and/or trustee, and prospective employers.[xx]
f.) Interests in securities: The CFR specifically addresses the potential conflicts that may arise out of interests in securities, such as stock holdings. The guidelines provided for in the CFR include:
(1) De minimis exemption: This exemption applies to publicly-traded or long-term Federal/municipal securities. The CFR states that persons having holdings in the specific parties involved of $5,000 or less or holdings in the affected companies of $25,000 or less will be allowed to participate in the proceedings of the advisory committee. (Exhibit 53) These financial interests are deemed to be of low involvement and do not require a waiver, but a simple disclosure on the forms required by the particular agency or department.
(2) Employment exemption: Under the DFR, SGEs may participate in the advisory committee discussions on matters of general applicability so long as the otherwise disqualifying financial interest arises only from the committee members non-Federal employment or prospective employment and so long as the matter does not have a special or distinct effect on the employee or employer other than as part of a class. In other words, under these circumstances, employees will be granted an automatic waiver.
g.) Teaching, speaking and writing on subject of meeting: SGEs are prohibited from receiving compensation for teaching, speaking, and writing on subjects related to the employees official duties in the advisory committee.[xxi]
The Code also stipulates that an SGE may not participate in matters that are likely to have a direct and predictable effect on the financial interests of …a person with whom he has a covered relationship, including members of his household, close friends or employer.[xxii] This type of conflict requires that the member disclose the potential conflict and that said conflict be waived by the agency designee.
Section III
The Rotavirus and the Rotashield Vaccine
A. What is Rotavirus?
Rotaviruses cause acute gastroenteritis. Rotavirus gastroenteritis is a self-limiting, mild to severe disease characterized by vomiting, watery diarrhea, and low-grade fever. Infantile diarrhea, winter diarrhea, acute nonbacterial infectious gastroenteritis, and acute viral gastroenteritis are names applied to the infection caused by the most common and widespread “Group A rotavirus.”
Person-to-person spread through contaminated hands is probably the most important means by which rotaviruses are transmitted in close communities such as pediatric and geriatric wards, day care centers and family homes. Group A rotavirus is endemic worldwide. It is the leading cause of severe diarrhea among infants and children, and accounts for about half of the cases requiring hospitalization.
It is estimated that over 3 million cases of rotavirus gastroenteritis occur annually in the United States. In temperate areas, it occurs primarily in the winter, but in the tropics it occurs throughout the year.
Group B rotavirus, also called adult diarrhea rotavirus or ADRV, has caused major epidemics of severe diarrhea affecting thousands of persons of all ages in China. Group C rotavirus has been associated with rare and sporadic cases of diarrhea in children in many countries. However, the first outbreaks were reported from Japan and England.
The incubation period ranges from 1-3 days. Symptoms often start with vomiting followed by 4-8 days of diarrhea. Temporary lactose intolerance may occur. Recovery is usually complete. However, severe diarrhea without fluid and electrolyte replacement may result in severe diarrhea and death.
Childhood mortality caused by rotavirus is relatively low in the U.S. Estimates of death resulting from complications of rotavirus are from 20[xxiii] to 100 deaths per year. From 1979 through 1985, an average of 500 children died annually from diarrhea disease in the United States; an estimated 20% of these deaths were caused by rotavirus infection. Death rates for diarrhea disease were highest in the South and among black children less than 6 months of age. Many deaths and hospitalizations may be prevented by the aggressive use of oral rehydration therapy, which is underused. Children 6 months to 2 years of age, premature infants, the elderly, and the immuno-compromised are particularly prone to more severe symptoms caused by infection with Group A rotavirus. Outbreaks of Group A rotavirus diarrhea are common among hospitalized infants, young children attending day care centers, and elder persons in nursing homes.[xxiv]
B. Rotavirus Vaccine Development
Wyeth Lederle Vaccines and Pediatrics, a subsidiary of American Home Products was the first pharmaceutical company to come to market with a rotavirus vaccine. The Rotashield was approved by the Food and Drug Administration on August 31,1998. It was a Rhesus monkey-based live oral vaccine. Merck was also developing a rotavirus vaccine that was based on bovine cells. The National Institute of Allergy and Infectious Diseases was conducting research in rotavirus vaccine development. Smith Kline Beecham was also working on a rotavirus vaccine.
Wyeth-Lederle Vaccines and Pediatrics first filed their Investigational New Drug Application in August of 1987 for the Rotashield vaccine. This vaccine had an overall relative efficacy of 49% to 83% for four strains of rotavirus.
C. Timeline for Vaccine Approval and Universal Use Recommendation
Date Individual or Organization Action August 1, 1987 Wyeth Lederle Filed Investigational New Drug (IND) Application to the FDA December 9, 1994 Fred Clark, Paul Offit, Stanley Plotkin (Inventors); Wistar Institute of Anatomy and Biology and Children’s Hospital of Pennsylvania (Assignees) Filed U.S. Patent for Rotavirus reassortant vaccine. Application number 353547 June 1, 1995 Fred Clark, Paul Offit, Stanley Plotkin (Inventors); Wistar Institute of Anatomy & Biology and Children’s Hospital of Philadelphia (Assignees) Filed U.S. Patent for rotavirus reassortant vaccine. Application number 456906 May 6, 1997 Fred Clark, Paul Offit, Stanley Plotkin (Inventors); Wistar Institute of Anatomy and Biology and Children’s Hospital of Pennsylvania (Assignees) Awarded U.S. Patent # 5,626,851 for Rotavirus Reassortant vaccine. December 12, 1997
VRBPAC (FDA) The committee voted to recommend that the FDA license the Rotashield vaccine. February 11, 1998
ACIP (CDC) The committee voted to include the statement “Routine Vaccination” in the ACIP statement. June 25, 1998
ACIP (CDC) The committee voted to include the short version of the ACIP statement regarding post-marketing surveillance. August 31, 1998 FDA
FDA approved the Rotashield vaccine. October 1, 1998 Wyeth-Lederle
Distribution of the Rotashield began. October 21-22, 1998
ACIP (CDC) The committee voted to add the rotavirus vaccine to the Vaccines For Children Program. January 15, 1999
CDC
ACIP published its recommended immunization schedule in the Morbidity and Mortality Weekly Report (MMWR). February 17-18, 1999
ACIP (CDC) The committee voted in favor of recommending immunization of infants who have diarrhea at the time presented for immunization. February 17-18, 1999
ACIP (CDC) The committee voted to include infants born prematurely under guidelines for routine immunization with a precaution to insure the infant was at least six weeks of age, leaving a nursery or no longer hospitalized, and clinically stable. March 19, 1999
CDC
CDC officially adopted recommendation for routine use of rotavirus vaccine as published in MMWR. May 1999
FDA
Ten cases of intussusception reported through the VAERS System. June 17, 1999
ACIP (CDC) The ACIP discussed intussusception reports to the Vaccine Adverse Event Reporting System (VAERS) July 16, 1999
CDC
MMWR published request to suspend use of Rotashield until further analysis of existing reports of intussusception. October 15, 1999 Wyeth-Lederle
A subsidiary of American Home Products Manufacturer voluntarily removed Rotashield from the U.S. market. October 22, 1999 ACIP (CDC) The Committee voted to rescind the Recommendation of the Rotashield Rotavirus Vaccine.
D. Severe Bowel Obstructions Tied to Rotashield Vaccine
A little more than one year after the Rotashield rotavirus vaccine was licensed by the Food and Drug Administration as a safe and effective vaccine, it was removed from the market due to adverse events. More than 100 cases of severe bowel obstruction, or intussusception, were reported in children who had received the vaccine were reported.
Rotashield was licensed by FDA on August 31, 1998. Distribution began on October 1, 1998. On January 1, 1999 there were zero cases of intussusception on the Vaccine Adverse Events Reporting System (VAERS). In May 1999 there were ten cases of intussusception reported in the VAERS. Data was received from the Northern California Kaiser active surveillance system and from statewide data case control in Minnesota in early June that supported a relationship between the Rotashield vaccine and intussusception. Dr. Jeffery P. Koplan, Director of the CDC was briefed for the first time on June 11, 1999. A subsequent meeting was held with Dr. Koplan and the CDC at which a decision was made to postpone any further use of the vaccine until further analysis was conducted. This was published in MMWR on July 16, 1999.
As of October 15, 1999, 113 cases of intussusception had been received. Nine of these reported cases were determined not to be intussusception. Of the remaining 102 cases of intussusception, 57 had received the vaccine. Of these, 29 required surgery, seven underwent bowel resection, and one five-month-old infant died after developing intussusception five days after receipt of the vaccine.[xxv] A case study was conducted that estimated that the risk of intussusception was increased by sixty percent among children who received the Rotashield.
It is alarming that it was known during clinical trials and the licensing process that there were increased incidences of intussusception in vaccinated infants. The topic was raised at a VRBPAC meeting and a reference to intussusception is listed in the ACIP recommendation, however, the committee apparently determined that the reported rate of 1 in 2010 was not to be statistically significant. The CDC continues to provide inconsistent information on their web site. One fact sheet, the Rotavirus Q & A, has not been updated since July 16, 1999 and does not provide a link to a more recent fact sheet. The fact sheet significantly plays down the seriousness of the adverse event and asserts that no association has been made.[xxvi] Another Rotavirus Vaccine Fact Sheet was updated on February 2, 2000 that indicates that the FDA and CDC confirmed the association between Rotashield and intussusception.
During the clinical trials, five children out of a total of 10,054 subjects suffered intussusception.[xxvii] If confirmed, the rate of intussusception would be 1 in 2010 children. According to the manufacturers package insert, the adverse event was considered statistically insignificant at 0.05%. Intussusception had not previously been associated with natural rotavirus infection.
Rotashield rotavirus vaccine was removed from the U.S. market in October 1999. Development of other rotavirus vaccines continues by Merck and others.
Section IV
Food and Drug Administration
Vaccines and Related Biological Products Advisory Committee
A. Vaccines and Related Biological Products Advisory Committee:
1. Description of the Committee:
The Vaccines and Related Biological Products Advisory Committee (VRBPAC) advises the Commissioner of the Food and Drug Administration in discharging her responsibilities as they relate to helping ensure safe and effective biological products, including vaccines.[xxviii] It reviews and evaluates the data concerning the safety, effectiveness, and the appropriate use of vaccines and related biological products. In short, the VRBPAC advises the FDA on whether or not to license new vaccines for commercial use.
2. Membership of the Committee:
The VRBPAC has 15 voting members, including the Chair, who are selected by the Commissioner of the FDA or her designee. The FDA seeks members who are “authorities” in the fields of immunology, pediatrics, infectious diseases and related fields. The charter also suggests that there be a member who is identified with consumer interests. VRBPAC meets approximately 6 times a year.
3. Terms:
VRBPAC members serve overlapping terms of four years. A member may serve after the expiration of the members term until a successor has taken office. Under the DHHS policy, members may not serve continuously for more than four years or more than eight years within a twelve year period. Additionally, members may not serve on more than one committee within the agency at the same time. Vacancies are announced at least once a year in the Federal Register. The selections are made by Dr. Linda Suydam, Senior Associate Commissioner of the FDA, who also considers and grants all conflict of interest waivers.
4. Temporary voting members:
Members of other scientific and technical FDA advisory committees — not to exceed 4 members (Exhibit 54) — may vote on the VRBPAC when: a.) expertise is required that is not available among current voting members or, b.) their presence is needed to comprise a quorum.
B. Conflict of Interest Review and Waivers by the FDA
1. Scope:
As discussed in Section I of this report, conflict of interest statutes and regulations generally prohibit the participation of advisory committee members in official matters where that person has a financial interest and their participation will have a direct and predictable effect on that interest.[xxix] Many factors are considered by the Department in determining whether a conflict of interest exists and, if it does, whether it may be waived to allow participation. A conflict may either be an actual or apparent conflict. An actual conflict is the situation where a direct, identifiable conflict exists. An apparent conflict is where there is an appearance of a lack of impartiality.[xxx]
2. Procedure:
There are many steps in the FDA’s procedure to clear potential conflict of interests in VRBPAC.
They include:
a. Prior to a scheduled VRBPAC meeting, FDA officials will review the agenda and other assignments. Entities with a financial interest in the matter to be discussed are identified by the staff of the Center for Biologics Evaluation & Research, as are the products to be used in conjunction with the product being reviewed, and competing products.
b. Advisory committee members are required to fill out a Confidential Financial Disclosure Statement (FDA form 3410) prior to each meeting.
c. FDA staff compares financial disclosure information compiled for each VRBPAC member with the issues on the agenda for the upcoming meeting to determine who has conflicts. Based on the information provided, the member can be found to have: a.) no conflict of interest, b.) a conflict of interest that is minimal and thus, justifiable, or c.) a conflict of interest so substantial than recusal or a waiver is the only course of action. If there is a substantial conflict of interest, it must be detailed. Some of the factors and criteria used in determining whether a waiver is appropriate include:
(i.) Agenda topic: Where the subject of the meeting is of Ageneral scientific presentations and not of particular products or to review research with no direct or predictable effect on outside interests, waivers are not needed.[xxxi]
(ii.) Net worth of member: The amount of the financial interest will be considered in relation to the net worth of the SGE.[xxxii]
(iii.) Employment: Situations where the SGE’s university employer has a grant or a contract with either the sponsoring company or any other affected companies will be taken into consideration during the waiver process.[xxxiii]
(iv.) Amount of grant or contract: The amount of the grant or contract given to the university employer of a member, as well as the member=s involvement (i.e. principal investigator, department chair) will be considered in whether the financial interest arises to the point of conflict. (Exhibit 53).
(v.) Competing products: The member’s financial interest in competing products or otherwise affected companies will be taken into consideration by the agency in determining whether a waiver may be granted.[xxxiv]
(vi.) Potential effect of committee recommendation: Members may not vote on any matter where a committee recommendation could benefit financially either the member or his/her immediate family. A waiver may not be granted where the member’s own research is involved.
(vii.) Industry consultant or advisor: The level of involvement of the member with either a sponsoring or an affected company, as measured by the amount of compensation received, will also be considered. (Exhibit 53).
(viii.) Patents, royalties and trademarks: As in the previous categories, the level of involvement of the particular member will be measured by the amount of compensation received from the sponsoring or affected companies. (Exhibit 53).
b. If the Director of the division determines that the member’s services are too important, despite a substantial conflict of interest, he must provide the necessary justification for a waiver. Where the financial interest is relatively large it is essential that the justification be particularly strong.[xxxv]
c. If a waiver is contemplated, it must be reviewed by FDA’s ethics staff who will make a recommendation to the approving official regarding the waiver. They may also consult with the Office of General Counsel in the Department or the Office of Government Ethics.
d. Final approval of waivers is given by Dr. Linda Suydam, Senior Associate Commissioner of the FDA. In addition to a full participation waiver, the Department may also grant:
i.) Limited Waivers: This waiver places restrictions on the member’s participation, such as no right to vote.[xxxvi] Potentially, a limited waiver could also restrict a member’s participation to answering factual questions about the matter being discussed by the committee.
ii.) Disclosure: In cases where the financial interest is not deemed to be substantial, it will be disclosed in the public record with the expectation that other participants will take them into consideration as they evaluate the opinions expressed by the member. The Agency in some cases deems that such disclosure is sufficient in addressing the potential for an actual or apparent conflict of interest.[xxxvii]
iii.) Recusal: Finally, members are expected to recuse themselves from the committee proceedings in cases where they deem that the financial interest may interfere with their ability to be impartial.
C. Problems identified with VRBPAC:
The Committee conducted an in-depth investigation of the VRBPAC from 1995 to present. As noted above, the approval and recommendation of the Rotashield vaccine for the treatment of rotavirus was chosen as a good example of the concerns that arise from the use of waivers by advisory committees. For the purposes of this report, we chose the VRBPAC’s December 12, 1997, meeting, at which the Rotashield vaccine received its initial approval.
This meeting was attended by 5 VRBPAC committee members, 5 temporary voting members and at least 3 consultants, in addition to both the FDA and the sponsor company’s representatives. Although Wyeth-Ayerst Laboratories (Wyeth Lederle Vaccines and Pediatrics) was the sponsoring company for the Rotashield vaccine, several other companies were deemed to be AAffected Companies by the FDA. These include: Merck, Virus Research Institute, and National Institute on Allergy and Infectious Diseases (NIAID). Advisory committee members, temporary voting members and consultants were screened for potential financial conflicts of interest with either the sponsoring or the affected companies. The decision to recommend approval of the license for the Rotashield was unanimous. The Government Reform Committee’s investigation of the VRBPAC’s Rotashield vaccine approval meeting raised several concerns:
1. Unanimous vote despite concerns raised: At the VRBPAC meeting, several members raised concerns about adverse effects that occurred at the rotavirus clinical trials. These included: intussusception, infant’s failure to thrive, and febrile reactions among others.
A statement by Dr. Fleming, a temporary voting member, summarizes the statements of many of the other voting members. He stated: “And as a result, I would ask the FDA to work with the sponsor to further quantitate what these serious side effects are — specifically the adverse effects, driven in particular by febrile illness — is inducing hospitalizations and what is that level of access. I still don’t feel like I have a good grasp of that at this point.” He proceeded to vote for the approval recommendation.[xxxviii]
2. Potential conflicts of interest of VRBPAC members: Four out of five members had conflicts of interest that necessitated waivers. Perhaps one of the major problems contributing to the overall influence of the pharmaceutical industry over the vaccine approval and recommendation process may be the loose standards that are used by the agency in determining whether a conflict actually exists. (Exhibit 53). In many cases, significant conflicts of interest are not deemed to be conflicts at all.
For this particular meeting, two members of the VRBPAC were excluded from the committee deliberations:
a.) Dr. Harry Greenberg: Dr. Greenberg was excluded from the deliberations as he is a patent holder of the Rotashield, the actual vaccine discussed at the meeting. He may have been present at the VRBPAC meeting, but it is not apparent that he participated in any way, including the open public session.
b.) Dr. Clements-Mann: It is not clear from the waiver process why she was excluded from participating in the proceedings.[xxxix] However, while Dr. Clements-Mann did not vote, she was present and did participate in the public session of the committee deliberations. Dr. Clements-Mann works for the Johns Hopkins University.
Five members out of fifteen members of the advisory committee were present in the deliberations:
c.) Dr. Patricia Ferrieri, Chair: She directed the discussion on the Rotashield vaccine. At the time of the proceedings, Dr. Ferrieri owned at about $20,000 of stock in Merck, an affected company and manufacturer of an upcoming rotavirus vaccine. This conflict was waived by the FDA as it was deemed to be of low involvement (Exhibit 56). Also, Dr. Ferrieri received a $135,000 NIAID grant for unspecified research on rotavirus[xl] for 1998-1999, after the committee voted to approve the Rotashield vaccine. It is not certain whether this grant was in negotiations at the time of the VRBPAC vote on Rotashield. Dr. Ferrieri received a full participation waiver.
d.) Dr. Caroline Hall: At the time of the VRBPAC meeting for approval of Rotashield, Dr. Hall’s employer, the University of Rochester, had a $9,586,000 contract with the NIAID for a rotavirus vaccine. As the original developer of the rotavirus vaccine, the NIAID subsequently licensed to Wyeth the rights to further develop the Rotashield vaccine. According to the conflict of interest waiver forms, neither Dr. Hall nor the principal investigator of the NIAID contract have evaluated the specific Rotashield vaccine. However, the same form states that it is unknown which rotavirus vaccine was licensed to Wyeth from NIAID. Dr. Hall was allowed to fully participate in the meeting.
e.) Ms. Rebecca Cole: The consumer representative on the VRBPAC committee at the time, Ms. Cole has been an ardent advocate for increased vaccinations after her son died of complications from his asthmatic condition and the chicken pox. As an advocate for vaccines, she has received both travel expenses and honoraria from Merck, the developer of the chicken pox vaccine, to appear in discussions advocating its use. Under the FDA standard, Ms. Cole did not need a waiver for participation.
f.) Dr. Kathryn Edwards: Dr. Edwards received a contract from Wyeth Lederle for $255,023 per year from 1996 to 1998 for the study of pneumococcal vaccines. She also had numerous grants and contracts with the NIAID, an affected company, for the following amounts: $206,750 per year from 4/1/95 to 3/1/98 to study TB vaccines; $673, 373 a year from 1996-2003 to study mucosal vaccines; and $86,279 from 1997-1998 to study acellular pertussis/cell mediate immunity. These contracts and grants were deemed to potentially appear to be a conflict, but were subsequently waived. Dr. Edwards was allowed full participation in the meeting.
g.) Dr. Mary Estes: At the time of the Rotashield approval meeting, Dr. Estes’ employer, Baylor College of Medicine, was receiving a large amount of funds for the development of rotavirus vaccines, including a $75,000 grant from American Home Products, the parent company of Wyeth-Lederle Vaccines and Pediatrics, and from the NIAID for $404,000 from 8/93 to 7/98. The FDA determined that the amount of funding is not large and represent[ed] a small portion of the University’s research budget. (Exhibit 61) Accordingly, this conflict was waived. Dr. Estes was also listed as the principal investigator for a grant from Merck for the development of a rotavirus vaccine. This conflict was also waived and Dr. Estes was given a full participation waiver for the meeting.
3. Use of temporary voting members:
An additional concern was raised by the liberal use of temporary voting members, particularly in the Rotashield approval meeting of VRBPAC. Of the ten (10) members allowed to vote in this meeting, only half (5) were standing members. The other half were temporary voting members. The VRBPAC charter states that the number of temporary members is normally not to exceed four members.[xli] This is bothersome as a meeting where a quorum cannot be constituted from the duly appointed members should be canceled until the quorum can be achieved. The temporary voting members appointed for this meeting were:
a.) Dr. Claire Broome: Senior Advisor to the Director for Integrated Health Information Systems at the Centers for Disease Control.
b.) Dr. Dixie Snider: Associate Director for Science at the Centers for Disease Control. Dr. Snider was, at the time, the Executive Secretary of the CDC’s Advisory Committee on Immunization Practices (ACIP).
c.) Dr. David Karzon: Professor at Vanderbilt University. Dr. Karzon is a frequent consultant and/or temporary voting member to the VRBPAC, voting on a variety of issues. While no apparent conflicts of interest were reported by Dr. Karzon, his employer, Vanderbilt University, receives extensive grants and contracts from pharmaceutical companies.
d.) Herbert DuPont: Professor at the University of Texas in Houston. No apparent conflicts of interest were reported.
e.) Thomas Fleming: Chair of Biostatistics at the University of Washington, Dr. Fleming has also been a frequent temporary voting member or consultant to the VRBPAC.
4. Conflicts of interest of consultants:
At least three consultants participated in the discussion of the Rotashield vaccine on December 12, 1997. They were:
a.) Dr. Neal Halsey: Dr. Halsey has been one of the leading investigators and advocates in the area of vaccines. In addition to numerous grants and contracts from different vaccine manufacturers, Dr. Halsey has received frequent reimbursements for travel expenses and honoraria from companies such as Merck. Importantly, at the time of the Rotashield approval meeting, Dr. Halsey was seeking start-up funds from most of the vaccine manufacturers for the establishment of an institute for vaccine safety at Johns Hopkins University, where he works. He has already received $50,000 from Merck and was awaiting funds from Wyeth Lederle (Exhibit 56). Dr. Halsey also participated in the rotavirus working group of the ACIP.[xlii] Also, Dr. Halsey was the Chair of the Committee on Infectious Diseases and representative of the American Academy of Pediatrics which, in conjunction with the CDC, sets and advertises the recommendations for schedules and dosages of immunizations. He was granted a waiver for participation,[xliii] participated during the morning session and then recused himself at the beginning of the afternoon session due to conflicts that were not disclosed in the minutes for the meeting. Finally, Dr. Halsey’s employer, Johns Hopkins University, is also the employer of Dr. Clements-Mann, who was excluded from the discussions.
b.) Dr. Yvonne Maldonado: No apparent conflicts were listed for Dr. Maldonado.
c.) Dr. John Modlin: At the time of the Rotashield approval meeting, Dr. Modlin owned approximately $26,000 in Merck stock, an affected company. He has also served on Merck’s Immunization Advisory Board from 1996 to the present. These financial interests were waived and he was allowed to extensively participate in the meeting although, as a consultant, he was not allowed to vote. Also, Dr. Modlin was at the time the Chairman of the ACIP and its rotavirus working group.
5. Balanced representation:
As previously discussed, the statutory requirement of balanced representation is one of the most controversial provisions of the FACA. The FDA has interpreted “balance” as diversity of geography, ethnicity, disciplines and gender. While it is questionable whether this standard guarantees the balance of points of view represented expressly required by the statute, it was interesting to see the high concentration of professors in pediatrics represented on the VRBPAC committee, particularly during the Rotashield discussion (Dr. Ferrieri, Dr. Karzon, Dr. Edwards, Dr. Modlin, and Dr. Halsey). Also, two of the voting members work for Vanderbilt University (Dr. Edwards & Dr. Karzon), while one member Dr. Clements-Mann (who, although excluded from voting, was able to participate in the open public hearing part of the meeting) and Dr. Halsey, both come from Johns Hopkins University. Two of the voting members (Dr. Broome and Dr. Snider) are CDC Federal employees. The overwhelming majority of members, both voting members and consultants, have substantial ties to the pharmaceutical industry.
6. Recurrent membership:
A troubling pattern is the recurrence of members, temporary voting members and consultants, year after year, despite term limits, which greatly limits the diversity of opinion that is sought in this type of committee.[xliv] After reviewing the VRBPAC rosters of members and consultants for the past few years, it becomes apparent that many of the members have frequently participated in committee proceedings for many years. Also, it is evident that there is a significant number of people who frequently participate in proceedings at both the FDA and the CDC, despite a policy that prohibits the simultaneous participation of members in more than one advisory committee within the agency.[xlv] In this particular meeting, at least four of the members (Dr. Broome, Dr. Snider, Dr. Modlin and Dr. Halsey) were intrinsically involved in the development of recommendations for the CDC. In other words, these persons influence the process of vaccine approval and recommendation. Dr. Halsey also chaired the American Academy of Pediatrics committee which helps set and advertise the schedule and dosage of recommended vaccines. Also, several of the temporary voting members frequently participate in VRBPAC’s meeting, without actually becoming members, thus severely limiting the diversity of participation and opinion.[xlvi] Other members are retained as temporary voting members and/or consultants once their four year term on the advisory committee has expired.[xlvii]
7. Timing of the proceedings:
A particularly troubling aspect of the deliberations on the Rotashield vaccine is the sequence of events. The ACIP Committee voted to recommend universal vaccinations of infants before the FDA licensure of the vaccine. Officials of the CDC acknowledge that they knew of no other instance where this has happened. As discussed before, during the December 12, 1997, VRBPAC vote to recommend the licensure of the Rotashield vaccine, a number of concerns were raised by some of the members with regard to the vaccine and its possible adverse effects. Although the VRBPAC unanimously approved the vaccine recommendation, some of the committee members votes were conditioned on the FDA’s ability to successfully resolve the areas of concern. However, before the FDA final licensure of the Rotashield vaccine in August 1998, the ACIP committee – as will be discussed in the ACIP section of this report- had already voted to recommend the mandatory universal use of the vaccine. This is troubling, not only because the vaccine had not yet been approved by the FDA, but because there were several areas of concerns that may not have been successfully addressed by the FDA, at the time of the ACIP vote.
Section V
Centers for Disease Control and Prevention
The Advisory Committee on Immunizations Practices
A. Practices and Procedures of the Advisory Committee on Immunization Practices (ACIP)
1. Purpose of the ACIP
ACIP provides advice and guidance on vaccine policy to the Secretary of DHHS, the Assistant Secretary for Health, and the Director of CDC. The ACIP develops written recommendations, subject to the approval of the Director of the CDC, for the routine administration of vaccines to the pediatric and adult populations, along with schedules regarding the appropriate periodicity, dosage, and contraindications applicable to the vaccines.
The recommendation for routine use of a vaccine is tantamount to a Federal mandate for vaccine use. HHS regulations require that all grants for childhood immunizations are subject to the States’ implementation of procedures to ensure routine vaccination. To receive federal funding the States must, among other things, require a plan to systematically immunize susceptible children at school entry through vigorous enforcement of school immunization laws.[xlviii]
Additionally, the ACIP has been given a mandate from Congress by the Omnibus Budget Reconciliation Act of 1993, to establish and periodically review and, as appropriate, revise a list of vaccines for administration to children in the Vaccine For Children Program (VFC), along with schedules regarding the appropriate periodicity, dosage, and contraindications applicable to the pediatric vaccines.[xlix] The VFC program provides for public purchase of vaccines for children without health insurance coverage. Under the VFC program, $474 million has been obligated to pay for the purchase of vaccines in fiscal year 2000.
2. Membership of the ACIP
The ACIP has three different categories of membership consisting of voting members, ex-officio members and liaison representatives.
a. Voting Members of the ACIP
The ACIP has twelve voting members, including the Chair, all approved by the Secretary of DHHS or his designee.[l] The ACIP members are selected based upon their expertise in the field of immunization practices.[li] The membership consists of U.S. citizens that have multi-disciplinary expertise in public health, and expertise in the use of vaccines and immunologic agents in both clinical and preventive medicine. The ACIP membership is required by FACA and agency guidelines to be fairly balanced in terms of point of view represented and the committee’s function. Specifically, the CDC attempts to select members from diverse backgrounds including geographic areas, gender, ethnic and minority groups, and the disabled.
(i.) Procedure for nomination to the ACIP
New members are nominated to the ACIP on an annual basis. Suggestions for membership to the committee are sought from a variety of sources including current and former ACIP members, professional societies, vaccine manufacturers and the general public. A panel of government officials screens the candidates for nomination to the committee and submits a slate of possible nominees to the director of the CDC. With approval of the CDC director, a nomination package is prepared for the Secretary of DHHS who makes the official appointments to the committee.
Committee members are nominated to serve for overlapping four-year terms. Members may serve after the expiration of their terms until their successors have taken office.[lii]
b. Ex Officio Members of the ACIP
The ACIP charter designates seven non-voting ex officio members to the committee from the following federal agencies:
1. Deputy Director, Division of Vaccine Injury Compensation, Bureau of Health Professions, Health Resources and Services Administration
2. Deputy Director for Scientific Activities, Office for the Assistant Secretary of Defense
3. Under Secretary for Health, Department of Veterans Affairs
4. Director, National Center for Drugs and Biologics, Food and Drug Administration (FDA)
5. Medical Advisor, Medicaid Bureau, Health Care Financing Administration (HVFA)
6. Director, Microbiology and Infectious Diseases Program, National Institute of Allergy and Infectious Diseases, HHS
7. Director, National Vaccine Program Office, CDC[liii]
Generally, designees of the officials listed above hold the ex officio positions. In contrast to regular voting members, who are expected to voice their personal opinions, ex-officio members are expected, to the extent possible, to represent the position and views of their sponsoring organizations.[liv]
c. Liaison Members:
In addition to the voting members and ex-officio members, the ACIP charter specifies 16 additional non-voting liaison representatives from professional societies and organizations responsible for the development and execution of immunization programs for children and adults. Like ex officio members, liaison members are expected, to the extent possible, to represent the positions and views of their sponsoring organizations. Liaison members are expected to contribute to committee discussions when issues of importance to their organizations are being discussed. These members can serve as appointed consultants to working groups and subcommittees to provide expert advise and apprise the working group of the position their organization endorses.[lv]
The liaison representatives to the ACIP consist of representatives from the following organizations:
1. American Academy of Family Physicians
2. American Academy of Pediatrics
3. American Association of Health Plans
4. American College of Obstetricians and Gynecologists
5. American College of Physicians
6. American Hospital Association
7. American Medical Association
8. Association of Teachers of Preventative Medicine
9. Canadian National Advisory Committee on Immunization
10. Hospital Infection Control Practices Advisory Committee, CDC
11. Infectious Diseases Society of America
12. National Medical Association
13. Pharmaceutical Research and Manufacturers of America
14. National Vaccine Advisory Committee
15. Biotechnology Industry Organization
16. Secretario de Prevencion y control de Enfermedades, Mexico
3. Decision-Making Process of the ACIP
a. Working Groups of the ACIP
When deemed appropriate by the Executive Secretary and the Chair of the ACIP, working groups may be formed to prepare draft policy recommendations to be submitted to the full ACIP for its consideration. The working groups must: 1) include one or more regular voting members, 2) include CDC staff members, 3) may include ex officio members and liaison representatives and other consultants. Vaccine manufacturer’s official representatives may not serve on working groups but, at the discretion of the chair, may be consultants to a working group.[lvi]
Generally, working groups range from six to fifteen members.[lvii] The working group is charged with reviewing all pertinent information relative to the recommendation for use of a vaccine. No notice is given to the public of working group meetings and discussions of the group are held in private. No minutes are taken at the meetings.
Upon drafting a proposed recommendation, the chair will submit the draft proposal to the ACIP for consideration. The ACIP members review the proposal and suggest revisions to the working group. This process is generally repeated numerous times. The process for making a final recommendation to the full ACIP generally takes eighteen to twenty-four months. The work that the working group does contributes in large part to the recommendations for use of a vaccine submitted to the Director for approval.
b. Full Meetings of the ACIP
Regularly scheduled meetings are usually held three times a year, at the discretion of the CDC, with meeting dates announced six to twelve months in advance. Notices of each meeting, along with agenda items that may be discussed, are published in the Federal Register in accordance with the requirements of FACA. Potential topics for ACIP consideration can be suggested by anyone, but are most often proposed by CDC program staff, ACIP members, and vaccine manufacturers.[lviii]
The meetings of the ACIP are held in public and are widely attended by representatives from government, industry, and other interested parties. Frequent votes are taken to decide on a given policy matter at hand. Whenever six or more members are not eligible to vote by reason of financial conflict or interest, the Executive Secretary has the authority to temporarily designate the ex-officio members as voting members.
c. Final Recommendations for Vaccine Use
ACIP recommendations are submitted to the agency for approval. Upon acceptance by the agency, ACIP recommendations are published in the Morbidity and Mortality Weekly Report Recommendations and Report published by the CDC. While the recommendations by the ACIP to the CDC are subject to agency approval, longtime CDC officials do not remember an ACIP recommendation that was not approved by the agency.[lix]
B. The ACIP Conflicts of Interest Resolution Process
1. Disclosure Requirements for ACIP Members As an SGE, every member of the ACIP is required to file the standard OGE form 450 confidential financial disclosure report once a year.[lx] New members of the ACIP must file a new entrant report no later than 30 days after assuming their position. All reports must cover the 12 months preceding the date of filing.
Members must report specific sources of earned income over $200 for the filer and $1,000 for the filer’s spouse. ACIP members must report all honoraria received in excess of $200, along with the date services were provided. The $1,000 threshold for spousal earned income does not apply to honoraria, because of special concerns about that form of income.[lxi] They must also report all assets held for investment or the production of income with a fair market value greater than $1,000 at the end of the reporting period. The filer does not have to report the dollar amount or values for any asset or income.[lxii]
2. Reviewer’s Responsibilities
The ACIP Deputy Ethics Officer, Mr. Joseph Carter, is responsible for ensuring that the OGE 450 is completely and properly filled out. Specifically, the reviewer is required by the OGE to check for the completeness of the financial disclosure form and that each asset and source of income are listed separately.
3. ACIP Waiver Process
Waivers are granted to each and every member of the ACIP whether or not they have conflicts of interests listed on their OGE 450. The ACIP issues “limited” 208 (B)(3) waivers on an annual basis to members who have potential conflicts of interest. The waivers allow members to participate in all matters that come before the ACIP, with the provisos that: (1) members recuse themselves from voting on matters involving vaccine-related entities where they have a current direct financial interest and (2) that they publicly disclose all relevant financial interests at the beginning of each ACIP meeting.
The waiver states that under Section 208(a) the members are under statutory obligation to refrain from participating in any deliberation that involves a particular matter having a direct and predictable effect on a financial interest attributed to them. They provide that the deputy ethics counselor has the authority under 18 U.S.C. §208(b)(3) to grant a waiver permitting the ACIP member to participate in such matters as deemed appropriate.[lxiii]
Waivers are requested by the Executive Secretary of the ACIP, Dr. Dixie Snyder, Jr. CDC Legal Counsel Kevin Malone concurs that the waiver is appropriate and the Deputy Ethics Counselor, Mr. Joseph R. Carter, is responsible for approving the waiver. In interviewing these individuals, the Committee staff was told, “we generally give them to everyone…we give them out freely.” The CDC representatives explained, it is “the nature of the industry that they will have conflicts…we will allow you to participate if you disclose your conflicts…we will let you discuss but not vote.”[lxiv]
4. Work Sheets
The Executive Secretary prepares a work sheet prior to every ACIP meeting detailing the conflicts of interest that members may have pertaining to the topics on the agenda. The work sheet is only for his use and is not disclosed to the public. The documents are considered informal and are not saved by the CDC.
C. Problems Identified During the Committee’s Investigation
The Committee staff’s review of the ACIP’s consideration of the rotavirus vaccine identified serious weaknesses in the CDC’s policing of conflicts of interest on this advisory committee. On June 25, 1998, the ACIP voted to recommend the rotavirus vaccine for routine use in infants. In reviewing the minutes of ACIP meetings and the financial disclosure forms of the ACIP members, the Committee staff identified a number of troubling issues:
1. ACIP Members Do Not Fully Disclose Conflicts of Interest
Examination of ACIP members’ financial disclosure forms reveals that many members do not fill them out completely. CDC ethics officials conceded to Committee staff that they have been lax in compelling the ACIP members to provide complete and thorough information.[lxv]
a. Dr. Mary (Mimi) Glodé (Exhibits 3-15)
Dr. Glodé lists reviews of medical legal cases on her OGE 450 for 1996, 1997, 1998, 1099 at 5 per year for her and her spouse, but does not detail the law firms or clients for whom they do the legal work. She only discloses that the maximum income allowed by University of Colorado is $10,000 per year.
Dr. Glodé and her spouse have attended numerous conferences and received honoraria for their attendance. However, she does not list who the sponsors were in 1995, 1996, 1997, 1998, 1999. She states only that the honoraria given was from $500-$750 Per occurrence and were limited to five per year; her spouse does 5-10 per year as well.
On her 1996 FDA financial disclosure form she lists that she was a co-principal investigator on an $84,500 grant from Chiron to study the MGNIN C Vaccine, $10,000 of which was a part of her salary. The study lasted for fifteen months from 10/96-3/98. But on her CDC financial disclosure forms for 1997, 1998, and 1999, this funding was not mentioned as required. Furthermore, the conflict was not mentioned on the waivers granted to her by the CDC for the same years. According to the Federal conflict of interest statutes she would not be able to participate in any deliberations regarding Chiron before the ACIP.
b. Dr. Marie Griffin
Dr. Griffin doesn’t fill out a new form each year. She references previous year’s forms instead and adds any new items to the current year’s form. (Exhibit 18)
She lists “publicly traded stock,” but not the specific companies on her 10/6/94, 2/95, 6/9/96, and 10/20/97 OGE 450. This is not sufficient under the law. (Exhibit 16)
c. Dr. Paul Offit
Dr. Offit lists that he is a consultant to Merck on an attachment to his OGE 450, but does not disclose whether or not he received any remuneration for his services. (Exhibit 39)
d. Dr. Richard Clover
Dr. Clover lists legal fees paid by the law firm of O’Bryan, Brown, and Toner, but not their client. (Exhibit 1)
The CDC informed the Committee staff that they have been unhappy with the OGE 450 and are working on a supplemental form. They stated that they wanted a form that was more specific and easier to fill out. Two years ago at the June 24-25, 1998, ACIP meeting, CDC Legal Counsel Kevin Malone stated his concerns to the ACIP:
“The 450 is a very frustrating form. All of us use the same form too and it is very difficult to even figure out what it is you should be disclosing. One of the things we’ve talked about is producing a supplementary form that would more explicitly lay out types of issues because certainly if we’re going to be in a position that we have to be announcing these interests, we would also need to feel a little bit more confident, I think that everything is being reported.”[lxvi]
However, two years later, the supplemental form has yet to be put into use.
2. Every Member of the ACIP is Granted a 208 (B) Waiver for the Entire Year
The CDC grants blanket waivers to the ACIP members each year that allow them to deliberate on any subject, regardless of their conflicts, for the entire year. In contrast, the FDA grants waivers on a meeting by meeting basis, taking into consideration the issues on the agenda and the affected companies discussed. Moreover, the FDA provides a list of parties that will be affected by their vote so their members clearly understand when they can not participate.
The CDC’s policy of issuing annual waivers creates an environment where people do not take the conflict of interest issue as seriously as they should. This policy, in concert with sloppy monitoring of the completeness of members’ financial disclosure statements, allows for a clubby environment where ethical concerns are downplayed.
3. ACIP Members are Allowed to Vote on Vaccine Recommendations, Even When They Have Financial Ties to Drug Companies Developing Related or Similar Vaccines
Members of the ACIP are allowed to vote on a recommendation for one company’s vaccine even if they have financial ties to a competing firm developing a similar vaccine. For example, in the case of rotavirus vaccine, the vaccine before the advisory committee was developed by Wyeth-Lederle. However, Merck and Smithkline-Beecham had rotavirus vaccines under development. A recommendation for Wyeth-Lederle’s vaccine would help pave the way for future recommendations for the products of Merck and Smithkline-Beecham.
While ACIP members with ties to Wyeth-Lederle were not allowed to vote on recommendations for the rotavirus vaccine, those with ties to Merck and Smithkline-Beecham were allowed to vote. This stands in stark contrast to the policies of the FDA. In discussions with FDA staff on this specific issue they informed the Committee staff that when the VRBPAC is deliberating the licensure of a vaccine, a company is considered affected [an affected company is one with a direct interest] if they are direct competitors of the manufacturer of the vaccine being considered. They further clarified that that this policy was in place because of the competing interest of the affected company and not because of concerns about the release of proprietary information. Moreover, if a VRBPAC member has a direct interest with a competing firm they are automatically disqualified from participation.
At ACIP meetings from February 11, 1998, through June 17, 1999, there were eight votes related to the their approval of the rotavirus vaccine for routine use. Three of these votes were particularly notable. They include: (1) June 25, 1998 – The ACIP approved the statement recommending the rotavirus vaccine for routine use, (2) October 22, 1998 – The ACIP recommended the rotavirus vaccine be added to the Vaccines for Children Program, and (3) October 22, 1999-the ACIP rescinded its earlier decision to recommend the rotavirus vaccine.
a. Dr. John Modlin-Chair beginning 2/11/98 (Exhibits 35-37)
Dr. Modlin owned 600 shares of stock in Merck as listed on his OGE 450. He serves on Merck’s Immunization Advisory Board but receives no remuneration. Dr. Modlin informed committee staff that he divested his shares in Merck some time in 1999.
Dr. Modlin was the Chairman of the Rotavirus working group. He voted yes on eight different matters pertaining to the ACIPs rotavirus statement, including recommending for routine use and for inclusion in the VFC program.
b. Dr. Paul Offit (Exhibits 38-41)
Dr. Offit shares the patent on the Rotavirus vaccine in development by Merck and lists a $350,000 grant from Merck for Rotavirus vaccine development. Also, he lists that he is a consultant to Merck.
Dr. Offit began his tenure on ACIP in October of 1998. Out of four votes pertaining to the ACIP’s rotavirus statement he voted “yes” three times, including, voting for the inclusion of the rotavirus vaccine in the VFC program.
Dr. Offit abstained from voting on the ACIP’s rescission of the recommendation of the rotavirus vaccine for routine use. He stated at the meeting, “I’m not conflicted with Wyeth, but because I consult with Merck on the development of rotavirus vaccine, I would still prefer to abstain because it creates a perception of conflict.”[lxvii]
c. Dr. Fernando Guerra (Exhibits 30-31)
Dr. Guerra lists a Contract with Merck Vaccine Division from 2/99-8/99 on his OGE 450, and a donation of $25,000 by Merck, Pasteur Merieux Connaught, and Medimmune (5/11/99 supplement to OGE 450). Also, he has a Contract with Smithkline-Beecham as a Principal Investigator (pending 7/99).
Dr. Guerra voted yes on eight different matters pertaining to the ACIP’s rotavirus statement, including recommending for routine use and for inclusion in the VFC program.
d. Dr. Marie Griffin (Exhibits 16-29)
Dr. Griffin lists consultant fees (3/21/97) and a salary from Merck relating to her position as Chair of Merck’s Endpoint Monitoring Committee on her OGE 450 (5/12/98 & 1/22/98).
She also lists consulting fees and travel expenses paid by Merck. (Exhibit 22)
Her spouse is a consultant for American Cyanamid (5/12/98 disclosure). American Cyanamid and Wyeth-Lederle are Subsidiaries/divisions of American Home Products Corporation.
Dr. Griffin voted on seven different matters (yes six times and no once) pertaining to the ACIPs rotavirus statement, including recommending yes for routine use and for inclusion in the VFC program.
d. Dr. T. Chinh Le (Exhibits 32-34)
Dr. Le’s employer, Kaiser Permanente, is participating in vaccine studies with Merck, Wyeth-Lederle, and Smithkline-Beecham. Additionally, Dr. Le owns stock in Merck as reported on his OGE 450. Dr. Le abstained from voting on all but one issue related to the Rotavirus.
e. Dr. Richard Clover (Exhibits 1-2)
Dr. Clover lists educational Grants from Merck and Smithkline-Beecham on his OGE 450. He voted on seven different matters (six times and no once) pertaining to the ACIPs rotavirus statement, including recommending voting yes for routine use and for inclusion in the VFC program.
4. Members Who are Not Allowed to Vote on a Recommendation Due to Financial Conflicts are Allowed to Fully Participate in the Discussion Leading up to a Vote
The “limited” 208(B)(3) waiver process enacted by the CDC allowing for discussion in all matters before the ACIP by conflicted members appears to be in direct contradiction to common practice at other DHHS agencies.
As stated succinctly by the Congressional Research Service, “Clearly, the influence on Government policy from advice and persuasion during a “discussion” of a particular recommendation, immediately preceding a vote on that recommendation, is significant and is equal under the law, to participating in a particular recommendation by way of voting for or against that recommendation.”[lxviii]
a. Inappropriate Statements by ACIP Members Undoubtedly Influence the Process
This is evidenced by several exchanges between Dr. T. Chinh Le and members of the ACIP. At one point during deliberations on the rotavirus vaccine, he said, “if I were to vote for this, I would vote for this routine immunization” and went on to encourage a two-dose regimen for the vaccine.[lxix] Moreover, at the June 1998 ACIP, meeting during which they approved the statement for routine use of the rotavirus vaccine, he said he “feels very privileged to be able to participate in a discussion that he cannot vote on . . . Hopefully, that perhaps what I will say will influence the people who can vote [referring to ex officio members] for me if I cannot vote.” When Committee staff queried CDC ethics officials regarding these statements, they acknowledged that they were inappropriate, and that they had discussed the issue with Dr. Le.
Dr. Le abstained from all but one vote related to the rotavirus vaccine because of significant conflicts of interest as stated earlier in this report. He did, however participate extensively in deliberations on the rotavirus vaccine and was a member of the rotavirus working group.
CDC conflict of interest policies are contrary to those of both the FDA, as cited earlier in this report, and that of the National Institutes of Health (NIH). The Office of Federal Advisory Committee Policy (OFACP) at NIH clearly states that a 208 (B)(3) waiver “is considered a ‘general’ waiver, in that it allows participation in matters that affect all institutions, or types of institutions, similarly. Even with a general waiver, however SGEs must disqualify themselves from participation in all matters that specifically and uniquely affect their [particular] financial interest.”[lxx]
5. Liaison Representatives Don’t have to Disclose Financial Conflicts of Their Organizations
Liaison representatives to the ACIP are not considered SGEs by the CDC.[lxxi] As such, they are exempted from the Federal conflict of interest statues the financial disclosure process. In the process of investigating events leading up to the approval of the rotavirus vaccine, the Committee staff has learned that the relationship between liaison members and the ACIP is substantially more formal than described by the CDC.
ACIP liaison members provide more than the just the opinions of their organization to the advisory committee’s process. Their role of the liaison representatives is more like that of a de facto SGE than an advisory representative. They are central to the process of creating recommendations for vaccine use by the ACIP. As official voting members of working groups that write draft recommendations for the committee’s consideration, they are under routine supervision by CDC staff and have meetings in government offices. Moreover, their advice is solicited frequently by CDC personnel on issues where their organization has a financial interest.
In a cursory review of publicly available references and an internet search, the Committee staff was able to find that the following organizations that the ACIP liaison representatives represent have ties to numerous vaccine manufacturers.
a. American Academy of Family Pediatrics
Abbott Laboratories, American Home Products Corporation, Aventis, Bayer Corporation, bioMerieux, Boehringer Ingelheim Chemicals Co., Bristol-Myers Squibb Company, Eli Lilly and Company, Forest Laboratories, G.D. Searle & Co., Glaxo Wellcome plc, Janssen Pharmaceutica, Lederle Laboratories, Merck & Co., Muro Pharmaceuticals, Novartis, Novo Nordisk A/S, Ortho-McNeil Pharmaceuticals, Otsuka America Pharmaceutical, Inc., Pasteur Merieux Connaught, Pfizer, Inc., Pharmacia, Schering AG, Schwarz Pharma, Inc., SmithKline Beecham, Solvay S.A., Warner-Lambert Company, and Wyeth-Ayerst Laboratories .[lxxii]
b. American Academy of Pediatrics
Abbott Laboratories, Astra, Merck & Co., Pasteur Merieux Connaught, Pfizer, Inc., and SmithKline Beecham.[lxxiii]
c. American College of Obstetricians and Gynecologists
Berlex Laboratories, Eli Lilly and Company, Novartis, Ortho McNeil Pharmaceutical, Pharmacia, Schering AG, and Wyeth-Ayerst.[lxxiv]
d. American Medical Association
Aventis, Glaxo Wellcome plc, Merck & Co., Pfizer, and Shering AG.[lxxv]
e. Infectious Disease Society of America
Aventis and Bristol-Myers Squibb Company.[lxxvi]
f. Biotechnology Industry Organization
Merck & Co., Wyeth-Ayerst and many other pharmaceutical companies.[lxxvii]
g. Pharmaceutical Research and Manufacturers of America
6.The Use of Working Groups is Contrary to the FACA (Exhibit 71)
a. Members of the Rotavirus Working Group of the ACIP
The ACIP rotavirus work group was responsible for creating the statement recommending universal use of the rotavirus vaccine. The working group has ten members, seven of whom have identifiable conflicts of interest with vaccine manufacturers or vaccine interest groups. The group’s meetings were held in private with no minutes or records of the proceedings taken. It appears that members who were not allowed to vote because of conflicts of interest with Wyeth-Lederle, such as Dr. Le, were allowed to work extensively on the recommendation for a long period of time in the working group.
The broad ability to grant waivers from the federal conflict of interest statutes was specifically enacted because of the statutory requirements and safeguards of the FACA. FACA requires that advisory committees hold public meetings, except in unusual circumstances. As such, deliberations of advisory committees are open to the most exacting public scrutiny. These requirements are to ensure public scrutiny of advisory committees operations and ensure that it is not a secretive or hidden vehicle for special interest influence.[lxxviii] The ACIPs prolific use of working groups to draft vaccine policy recommendations outside the specter of public scrutiny opens the door to undo special interest access.
i. John Modlin, M.D., Chairman
Chinh T. Le, M.D.
David W. Fleming, M.D
ACIP Voting Members
Dr. Le has conflicts with Wyeth Lederle and Smithkline-Beecham and Dr. Modlin has a conflict with Merck as described in this report.
ii. Roger I. Glass, M.D., Ph.D.
Joseph S. Bresee, M.D.
Centers for Disease Control and Prevention
National Center of Viral and Rickettsial Diseases
National Center for Infectious Diseases
iii. Margaret Rennels, M. D.
Department of Pediatrics, University of Maryland
Her employers website states that she participated in virtually all phases of the testing of the licensed rotavirus vaccine[lxxix] Also, she is affiliated with U.S. Rotavirus Efficacy Group[lxxx]
iv. Richard Zimmerman, M.D.
American Academy of Family Physicians (AAFP)
The AAFP has conflicts with numerous vaccine manufacturers as described in this report.
v. Neal A. Halsey, M.D.
American Academy of Pediatrics
At the time of the rotavirus approval meeting, Dr. Halsey was seeking start-up funds from most of the vaccine manufacturers for the establishment of an institute for vaccine safety at Johns Hopkins University, where he works. He has already received $50,000 from Merck and was awaiting funds from Wyeth Lederle. (Exhibit 56) He has received frequent reimbursements for travel expenses and honoraria from companies such as Merck.
Dr. Halsey Serves on the advisory board to the Immunization Action Coalition, an advocacy group funded by vaccine makers including: Aventis Pasteur, Chiron Corporation, Glaxo Wellcome, Merck & Co., Nabi, North American Vaccine, SmithKline-Beecham, Wyeth-Lederle Vaccines.[lxxxi]
vi. Peter Paradiso, Ph.D.
Lederle-Praxis Biologicals Division
Wyeth-Lederle Vaccines and pediatrics
vii. Florian Schodel, M.D.
Office for Clinical Vaccine Research
Merck Research Labs
7. ACIP is not Fairly Balanced in terms of the Points of View Represented
According to section 5 of FACA, membership on an advisory committee must be “fairly balanced in terms of points of view represented and the functions to be performed . . . ” and the advice and recommendations of the advisory committee cannot be “inappropriately influenced by the appointing authority or by any special interest.”
The absence of any consumer advocates on the ACIP has resulted in an advisory committee that is inherently not “fairly balanced.” It is clear to the Committee that the intent of the FACA was for individuals who are affected by the work of the ACIP, in this case vaccine recipients, to have significant representation on the committee.
The ACIP’s use of ex officio members, who are all government employees, in a voting capacity contradicts the notion of an advisory committee. Advisory committees are intended to provide independent information and advice to the government. In discussions with CDC staff, the Committee was informed that there are no records of an ex officio member ever voting no on an issue before the ACIP. This policy encourages a system where government officials make crucial decisions affecting American children without the advice and consent of the governed.
Congress sought to eliminate “the danger of allowing special interest groups to exercise undue influence upon the Government through dominance of advisory committees which deal with matters in which they have vested interests.”[lxxxii] However, the extensive use of working groups, in which conflict of interest procedures do not appear to be implemented, and the automatic waivers given to every advisory committee member, along with the absence of consumer representation, appear to thwart this goal.
Section VI
Recommendations
As a result of the review of the ACIP and VRBAC practices, the following Committee has the following recommendations to the Department of Health and Human Services:
1. Individuals who serve on advisory committees involving vaccines should have no financial ties to vaccine manufacturers.
2. Public participation on ACIP and VRBAC needs to be increased substantially.
3. Conflict of Interest waivers should be used more stringently.
4. A balance of policy perspectives should be incorporated into consideration of appointments of committee members.
5. Any level of stock ownership in vaccine manufacturers should not be allowed by committee members.
6. Department personnel need to insure that all documentation is fully and adequately completed.
7. Full explanation of participation as expert witnesses in legal cases needs to be a part of financial disclosures.
8. Individuals who have patents for vaccines for the same disease under discussion should not be allowed to participate in the discussion or vote of ACIP or VRBAC.
9. Individuals who are developing vaccines for the same disease under discussion should be not be allowed to participate in the discussion or vote of ACIP and VRBAC.
10. Working groups should be replaced by fully constituted Subcommittees on both the VRBAC and ACIP.
11. Individuals should not be allowed to participate on two DHHS advisory committees at the same time.
12. Individuals should not serve excessively long terms on a committee.
13. The FDA should reconsider its policy on using temporary voting members.
14. ACIP should not consider making a recommendation on a vaccine until it has been licensed by the FDA.
15. CDC should follow the same policy in identifying affected companies for vaccine discussions as the FDA does and exclude participation of any individual who has a conflict.
16. Organizations who send liaison members to participate in council meetings, should offer full disclosure of ties to the pharmaceutical industry.
17. The Department should review its policies and practices regarding conflicts of interest, participation on advisory committees, and terms of service, public participation, and balance of views and expertise.
[i] 5 U.S.C. app. II (1994).
[ii]Ensuring Coverage, Balance, Openness and Ethical Conduct for Advisory Committee Members Under the Federal Advisory Committee Act, 5 Admin. L.J. 231, Mary Kathryn Palladino, Spring, 1991.
[iii]5 U.S.C. app. II ‘7(c). The guidelines for the Food and Drug Administration=s advisory committee are set forth in 5 C.F.R. ‘2640 (1994)
[iv]5 U.S.C. app. II ‘2(b)(6) (1994).
[v]5 U.S.C., ’10 (b).
[vi]5 U.S.C., ‘5 (b)(2).
[vii]5 U.S.C., ‘5(b)(3).
[viii]18 U.S.C. ”202-209.
[ix]18 U.S.C. ‘208.
[x]18 U.S.C. ‘208(b)(1).
[xi]18 U.S.C. ‘208(b)(2).
[xii]18 U.S.C. ‘208(b)(3).
[xiii]FACA amendments of 1989
[xiv]5 C.F.R. ‘2640.103(a)(1).
[xv]5 C.F.R. ‘2640.102(l).
[xvi]5 C.F.R. ‘2640.102(m).
[xvii]5 C.F.R. ‘2640.103(a)(3).
[xviii]Id.
[xix]Id. at (b).
[xx]Id. at (c)(5).
[xxi]5 C.F.R. ‘ 2635.807.
[xxii]5 C.F.R. ‘2635.502.
[xxiii] Minutes of ACIP meeting, October 22, 1999 at 51.
[xxiv] Bad Bug Book, U.S. Food & Drug Administration, Center for Food Safety & Applied Nutrition, Foodborne Pathogenic Microorganisms and Natural Toxins Handbook, Chapter 33
http://vm.cfsan.fda.gov/~mow/chap33.html.
[xxv] Minutes of ACIP meeting, October 22, 1999, 56-57.
[xxvi] CDC’s Rotavirus Q&A http://www.cdc.gov/nip/Q&A/genqa/Rotavirus.htm.
[xxvii] Rotashield Package Insert, Wyeth-Ayerst, 13.
[xxviii]VRBPAC charter, DHHS, 12/21/99.
[xxix]5 C.F.R. ‘2640.103(a).
[xxx]Waiver Criteria Document 2000, FDA, 2. (Replacing the AWaiver Criteria Document (1994).@)
[xxxi]Id. at 19.
[xxxii]Id. at 23.
[xxxiii]Id. at 20. Where the grant or contract relates to the subject matter of the committee discussion, an actual conflict may arise. In situations where the grant or contract is unrelated to the product at issue, an appearance problem may arise. In either situation the conflict of interest may be waived and the member allowed to participate.
[xxxiv]Id. at 17.
[xxxv]Policy and Guidance, Handbook for FDA Advisory Committees, 12.
[xxxvi]Waiver Criteria Document (2000), FDA, 19.
[xxxvii]Id.
[xxxviii] VRBPAC “Rotashield” rotavirus vaccine approval meeting transcript, page 210, December 12, 1997.
[xxxix]A copy of the waiver forms have not been provided to the Committee.
[xl]The NIAID is the original developer of the Rotashield and other rotavirus vaccines. According to the FDA, as stated in Dr. Caroline Hall’s Conflict of Interest Waiver form, Wyeth received the rights to further develop the Rotashield from NIAID and it is unknown which rotavirus vaccine was licensed to Wyeth by the NIAID.
[xli]Please see VRBPAC Charter. Exhibit 54
[xlii]See further discussion of the ACIP rotavirus working group in the ACIP section of this report. Section IV
[xliii]Consultants may be allowed to participate in the committee’s discussion, but may not vote, unless designated a temporary voting member in advance of the meeting.
[xliv]According to the DHHS policy, members cannot serve for more than eight combined years within a period of 12 years.
[xlv]Letter from Mr. David Doleski, FDA, to the Government Reform Committee (March 30, 2000), stating that the DHHS policy states that Federal advisory committee members will not: ..serve on more than one committee within an agency at the same time.
[xlvi]Some of the frequent temporary members and consultants in the past few years include: Dr. Fleming (at least 4 meetings from 7/96 to 12/97); Dr. Karzon (at least 5 meetings between 4/96 until 9/99); Dr. Snider (at least 4 meetings in 1997, before becoming a standing member in 1998); Dr. Broome ( 8 meetings from 4/96 to 12/97); Dr. Diane Finkelstein (consultant in at least 5 meetings from 4/96 to 12/97, when she became a standing member); Dr. Theodore Eickhoff (consultant on at least 8 meetings from 4/96 to 9/99); Dr. Rob Breiman (4 meetings from 11/98 to 9/99).
[xlvii] For example, Dr. Ferrieri (at least 4 meetings past her appointment ); Dr. Gregory Poland (at least 2 meetings past his appointment); Dr. Alison O’Brien ( at least 3 meetings past her appointment) and Ms. Rebecca Cole (1 meeting past her appointment).
[xlviii] 42 C.F.R. §51b.204
[xlix] Section 1928 of the Social Security Act (42 U.S.C. § 1396s), as added by Section 13631 of the Omnibus Budget Reconciliation Act of 1993
[l] ACIP Charter, May 3, 1998 as approved by Claire Broome, Acting Director CDC (Exhibit 72)
[li] ACIP Charter, May 3, 1998 as approved by Claire Broome, Acting Director CDC, 2
[lii] ACIP Charter, May 3, 1998 as approved by Claire Broome, Acting Director CDC, 3
[liii] ACIP Charter, May 3, 1998 as approved by Claire Broome, Acting Director CDC, 2
[liv] The Advisory Committee on Immunization Practices, Centers for Disease Control and Prevention, Policies and Procedures for Development of Recommendations for Vaccine Use and for the Vaccines for Children, January 2000, 4 (Exhibit 73)
[lv] ACIP Charter, May 3, 1998 as approved by Claire Broome, Acting Director CDC, 4
[lvi] The Advisory Committee on Immunization Practices, Centers for Disease Control and Prevention, Policies and procedures for Development of Recommendations for Vaccine Use and for the Vaccines for Children, January 2000.
[lvii] Telephone interview of Dr. John Modlin (June 9, 2000).
[lviii] The Advisory Committee on Immunization Practices, Centers for Disease Control and Prevention, Policies and Procedures for Development of Recommendations for Vaccine Use and for the Vaccines for Children, January 2000.
[lix] Interview of Dr. Dixie Snider, Mr. Kevin Malone and Mr. Joe Carter (June 1, 2000).
[lx] 5 C.F.R. § 2634.904(b).
[lxi] OGE Form 450: A review Guide, U.S. Office of Government Ethics, 15 (September 1996).
[lxii] OGE Form 450: A review Guide, U.S. Office of Government Ethics, 15 (September 1996).
[lxiii] Cited from a several examples of waivers provided by the CDC to the Government Reform Committee.
[lxiv] Interview of Dr. Dixie Snider, Mr. Kevin Malone and Mr. Joe Carter (June 1, 2000).
[lxv] Interview of Dr. Dixie Snider, Mr. Kevin Malone and Mr. Joe Carter (June 1, 2000).
[lxvi] ACIP Meeting June 24, 1998, 41.
[lxvii] ACIP Meeting, October 22, 1999.
[lxviii] Conflicts of Interest and the Disqualification of Federal Advisory Committee Members, Congressional Research Service Memorandum, June 6, 2000.
[lxix] ACIP Meeting Minutes, February 11 and 12, 1998.
[lxx] Ethics Rules for Advisory Committee Members, for committee members appointed to serve on HHS advisory committees as SGEs, NIH Office of Federal Advisory Committee Policy (OFACP), 4, http://www1.od.nih.gov/cmo/sge.htm.
[lxxi] Interview of Dr. Dixie Snider, Mr. Kevin Malone and Mr. Joe Carter (June 1, 2000).
[lxxii] http://www.aafp.org.
[lxxiii] http://www.aap.org.
[lxxiv] http://www.acog.org; http://www.figo2000.com/sponsors.cfm.
[lxxv] http://www.ama-assn.org.
[lxxvi] http://www.idsociety.org/pd/grants_toc.htm.
[lxxvii] http://www.bio.org.
[lxxviii] Conflicts of Interest and the Disqualification of Federal Advisory Committee Members, Congressional Research Service Memorandum, June 6, 2000.
[lxxix] http://som1.umaryland.edu/research.html.
[lxxx] ACIP Meeting, February 13, 1997.
[lxxxi] http://www.immunize.org/admin/funding.htm.
[lxxxii] FAC Standards ACT, supra note 10, at 6, reprinted in FACA Source Book, supra note 2, at 276, citing Hearings on H.R. 4383 Before the Legal and Monetary Affairs Subcommittee. Of the House Comm. On Government Operations, 92 Cong., 2d Sess., at 13-55 (1971), reprinted in 1972 U.S. Code Cong. & Admin. News 3434-76.
Committee on Government Reform
2157 Rayburn House Office Building
Washington, DC 20515
(202) 225-5074
Filed under: ADHD, Aspergers, autism, Child Health Safety, Hannah Poling, John Poling, MMR, vaccine, vaccine court, Vaccine Damage, Vaccines | Tagged: ADHD, Aspergers, autism, CDC, Centers for Disease Control, Child Health Safety, Disease Statistics, fraud, Hannah Poling, John Poling, MMR, research fraud, vaccination, vaccine, vaccine court, Vaccine Damage, Vaccines | 14 Comments »













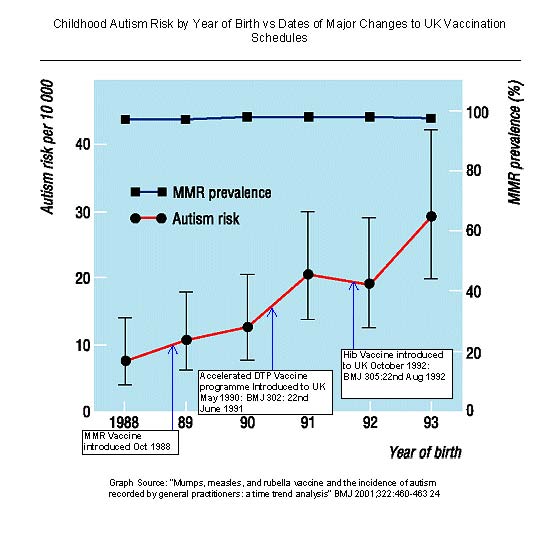


 Lothar Moll
Lothar Moll Lucy Martens
Lucy Martens Simon Modery
Simon Modery David Hason
David Hason





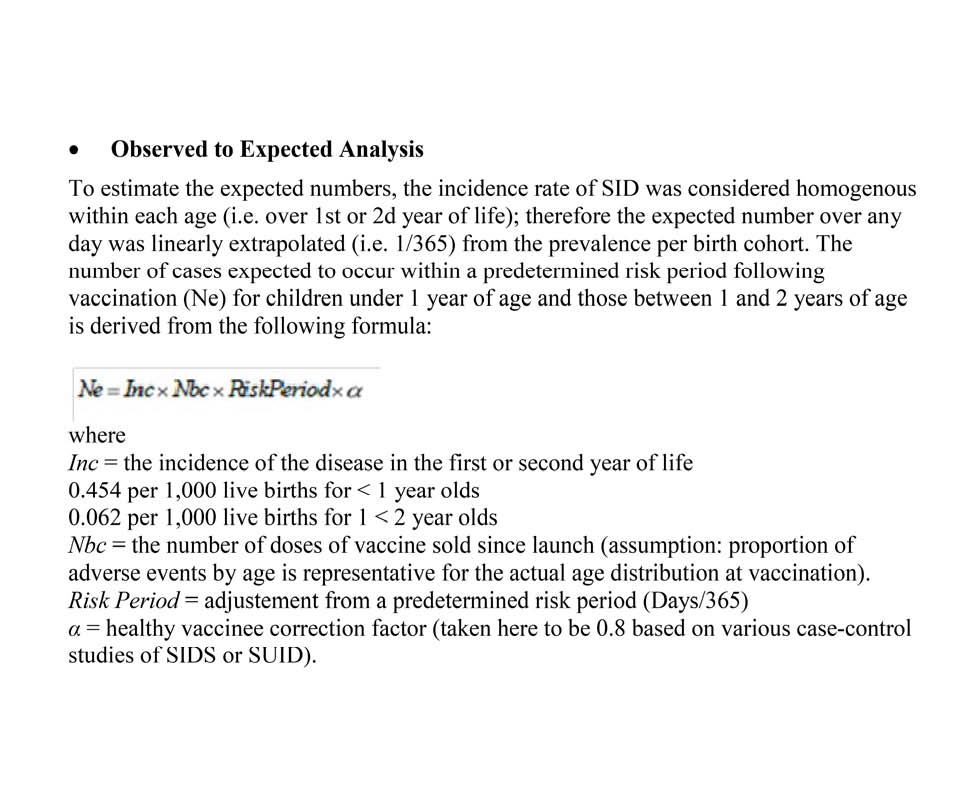



 Paul Morgan
Paul Morgan  Dragonblaze
Dragonblaze  Nat
Nat  Bongo B
Bongo B  Sisyphus
Sisyphus 



























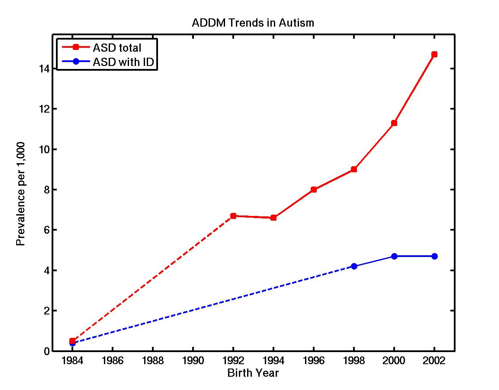
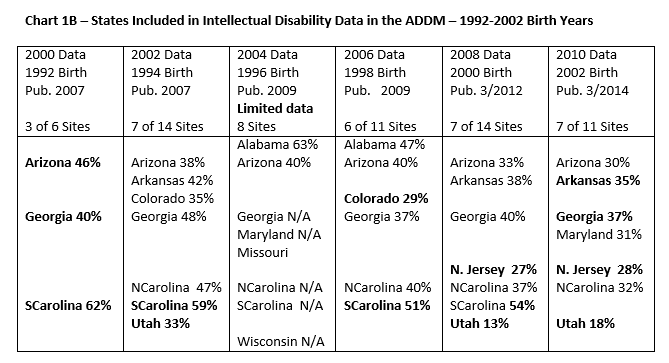



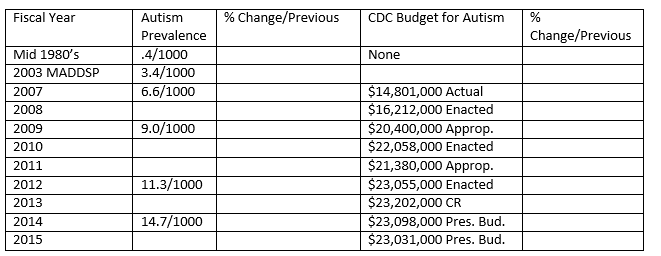








































 Some are calling this “‘compromise’, because most things in Montpelier are about ‘compromise’.” I disagree.
Some are calling this “‘compromise’, because most things in Montpelier are about ‘compromise’.” I disagree.











































")







In our post above noting direct censorship of public facts by The Guardian perhaps we should have added “Follow the Money”.
GUARDIAN & BRITISH MEDICAL JOURNAL
Guardian partners with British Medical Journal Group for online first Tuesday 3 March 2009 00.00 GMT
BRITISH MEDICAL JOURNAL & DRUG INDUSTRY
The Editor in Chief of the British Medical Journal was forced to make an embarrassing correction regarding the BMJ’s own failures to disclose its conflicting financial interests in the drug industry.
Here is the correction forced ultimately by online criticism from New York charity The Alliance for Human Research Protection:-
However, this also still fails to mention the most glaring conflict of all, which it all – BMJ’s business partnership with Merck through their information arm, Univadis (‘MSD signs partnership with BMJ group’).