| System Organ Class |
Category A to E |
Reported event (Preferred Term) |
Number of cases
|
|
A. Injection-site reactions |
Pain in extremity 485 |
485
|
|
A. Injection-site reactions |
Injection site swelling 113 |
113
|
|
A. Injection-site reactions |
Oedema peripheral 109 |
109
|
|
A. Injection-site reactions |
Limb discomfort 106 |
106
|
|
A. Injection-site reactions |
Hypoaesthesia 105 |
105
|
|
A. Injection-site reactions |
Injection site erythema 85 |
85
|
|
A. Injection-site reactions |
Injection site pain 81 |
81
|
|
A. Injection-site reactions |
Erythema 45 |
45
|
|
A. Injection-site reactions |
Paraesthesia 37 |
37
|
|
A. Injection-site reactions |
Skin discolouration 33 |
33
|
|
A. Injection-site reactions |
Injection site rash 32 |
32
|
|
A. Injection-site reactions |
Injection site mass 29 |
29
|
|
A. Injection-site reactions |
Injection site reaction 26 |
26
|
|
A. Injection-site reactions |
Pain 23 |
23
|
|
A. Injection-site reactions |
Contusion 21 |
21
|
|
A. Injection-site reactions |
Musculoskeletal stiffness 21 |
21
|
|
A. Injection-site reactions |
Peripheral coldness 20 |
20
|
|
A. Injection-site reactions |
Local reaction 19 |
19
|
|
A. Injection-site reactions |
Injection site inflammation 18 |
18
|
|
A. Injection-site reactions |
Injection site warmth 18 |
18
|
|
A. Injection-site reactions |
Pain in extremity 16 |
16
|
|
A. Injection-site reactions |
Local swelling 15 |
15
|
|
A. Injection-site reactions |
Sensation of heaviness 15 |
15
|
|
A. Injection-site reactions |
Injection site haematoma 12 |
12
|
|
A. Injection-site reactions |
Injection site pruritus 11 |
11
|
|
A. Injection-site reactions |
Rash macular 10 |
10
|
|
A. Injection-site reactions |
Oedema peripheral 9 |
9
|
|
A. Injection-site reactions |
Feeling cold 8 |
8
|
|
A. Injection-site reactions |
Injection site induration 8 |
8
|
|
A. Injection-site reactions |
Injection site nodule 8 |
8
|
|
A. Injection-site reactions |
Livedo reticularis 8 |
8
|
|
A. Injection-site reactions |
Swelling 8 |
8
|
|
A. Injection-site reactions |
Injection site anaesthesia 6 |
6
|
|
A. Injection-site reactions |
Injection site swelling 6 |
6
|
|
A. Injection-site reactions |
Muscular weakness 6 |
6
|
|
A. Injection-site reactions |
Myalgia 6 |
6
|
|
A. Injection-site reactions |
Neck pain 6 |
6
|
|
A. Injection-site reactions |
Pain 6 |
6
|
|
A. Injection-site reactions |
Rash 6 |
6
|
|
A. Injection-site reactions |
Erythema 5 |
5
|
|
A. Injection-site reactions |
Feeling hot 5 |
5
|
|
A. Injection-site reactions |
Injection site erythema 5 |
5
|
|
A. Injection-site reactions |
Pruritus 5 |
5
|
|
A. Injection-site reactions |
Cyanosis 4 |
4
|
|
A. Injection-site reactions |
Feeling abnormal 4 |
4
|
|
A. Injection-site reactions |
Injection site infection 4 |
4
|
|
A. Injection-site reactions |
Musculoskeletal stiffness 4 |
4
|
|
A. Injection-site reactions |
Pallor 4 |
4
|
|
A. Injection-site reactions |
Sensory disturbance 4 |
4
|
|
A. Injection-site reactions |
Tenderness 4 |
4
|
|
A. Injection-site reactions |
Asthenia 3 |
3
|
|
A. Injection-site reactions |
Feeling hot 3 |
3
|
|
A. Injection-site reactions |
Inflammation 3 |
3
|
|
A. Injection-site reactions |
Injection site discharge 3 |
3
|
|
A. Injection-site reactions |
Injection site discolouration 3 |
3
|
|
A. Injection-site reactions |
Injection site irritation 3 |
3
|
|
A. Injection-site reactions |
Injection site reaction 3 |
3
|
|
A. Injection-site reactions |
Injection site urticaria 3 |
3
|
|
A. Injection-site reactions |
Injection site vesicles 3 |
3
|
|
A. Injection-site reactions |
Limb immobilisation 3 |
3
|
|
A. Injection-site reactions |
Musculoskeletal pain 3 |
3
|
|
A. Injection-site reactions |
Poor peripheral circulation 3 |
3
|
|
A. Injection-site reactions |
Sensory loss 3 |
3
|
|
A. Injection-site reactions |
Skin warm 3 |
3
|
|
A. Injection-site reactions |
Dry skin 2 |
2
|
|
A. Injection-site reactions |
Grip strength decreased 2 |
2
|
|
A. Injection-site reactions |
Hypoaesthesia 2 |
2
|
|
A. Injection-site reactions |
Injected limb mobility decreased 2 |
2
|
|
A. Injection-site reactions |
Injection site cellulitis 2 |
2
|
|
A. Injection-site reactions |
Injection site coldness 2 |
2
|
|
A. Injection-site reactions |
Injection site discolouration 2 |
2
|
|
A. Injection-site reactions |
Injection site mass 2 |
2
|
|
A. Injection-site reactions |
Injection site pain 2 |
2
|
|
A. Injection-site reactions |
Peripheral coldness 2 |
2
|
|
A. Injection-site reactions |
Pruritus 2 |
2
|
|
A. Injection-site reactions |
Sensory loss 2 |
2
|
|
A. Injection-site reactions |
Skin discolouration 2 |
2
|
|
A. Injection-site reactions |
Skin reaction 2 |
2
|
|
A. Injection-site reactions |
Skin reaction 2 |
2
|
|
A. Injection-site reactions |
Tenderness 2 |
2
|
|
A. Injection-site reactions |
Blister 1 |
1
|
|
A. Injection-site reactions |
Complex regional pain syndrome 1 |
1
|
|
A. Injection-site reactions |
Extensive swelling of vaccinated limb 1 |
1
|
|
A. Injection-site reactions |
Hyperaesthesia 1 |
1
|
|
A. Injection-site reactions |
Hyperaesthesia 1 |
1
|
|
A. Injection-site reactions |
Hypokinesia 1 |
1
|
|
A. Injection-site reactions |
Hypokinesia 1 |
1
|
|
A. Injection-site reactions |
Immobile 1 |
1
|
|
A. Injection-site reactions |
Impetigo 1 |
1
|
|
A. Injection-site reactions |
Injection site abscess 1 |
1
|
|
A. Injection-site reactions |
Injection site anaesthesia 1 |
1
|
|
A. Injection-site reactions |
Injection site coldness 1 |
1
|
|
A. Injection-site reactions |
Injection site discomfort 1 |
1
|
|
A. Injection-site reactions |
Injection site haematoma 1 |
1
|
|
A. Injection-site reactions |
Injection site haemorrhage 1 |
1
|
|
A. Injection-site reactions |
Injection site haemorrhage 1 |
1
|
|
A. Injection-site reactions |
Injection site joint movement impairment 1 |
1
|
|
A. Injection-site reactions |
Injection site joint pain 1 |
1
|
|
A. Injection-site reactions |
Injection site movement impairment 1 |
1
|
|
A. Injection-site reactions |
Injection site movement impairment 1 |
1
|
|
A. Injection-site reactions |
Injection site papule 1 |
1
|
|
A. Injection-site reactions |
Injection site paraesthesia 1 |
1
|
|
A. Injection-site reactions |
Injection site rash 1 |
1
|
|
A. Injection-site reactions |
Injection site scab 1 |
1
|
|
A. Injection-site reactions |
Joint swelling 1 |
1
|
|
A. Injection-site reactions |
Limb immobilisation 1 |
1
|
|
A. Injection-site reactions |
Local reaction 1 |
1
|
|
A. Injection-site reactions |
Local swelling 1 |
1
|
|
A. Injection-site reactions |
Lymphoedema 1 |
1
|
|
A. Injection-site reactions |
Mass 1 |
1
|
|
A. Injection-site reactions |
Mobility decreased 1 |
1
|
|
A. Injection-site reactions |
Muscle rigidity 1 |
1
|
|
A. Injection-site reactions |
Muscle spasms 1 |
1
|
|
A. Injection-site reactions |
Muscle tightness 1 |
1
|
|
A. Injection-site reactions |
Musculoskeletal pain 1 |
1
|
|
A. Injection-site reactions |
Nausea 1 |
1
|
|
A. Injection-site reactions |
Nodule 1 |
1
|
|
A. Injection-site reactions |
Pain of skin 1 |
1
|
|
A. Injection-site reactions |
Paraesthesia 1 |
1
|
|
A. Injection-site reactions |
Peripheral vascular disorder 1 |
1
|
|
A. Injection-site reactions |
Rash 1 |
1
|
|
A. Injection-site reactions |
Rash maculo-papular 1 |
1
|
|
A. Injection-site reactions |
Rash pruritic 1 |
1
|
|
A. Injection-site reactions |
Scab 1 |
1
|
|
A. Injection-site reactions |
Sensation of heaviness 1 |
1
|
|
A. Injection-site reactions |
Sensation of pressure 1 |
1
|
|
A. Injection-site reactions |
Tremor 1 |
1
|
|
A. Injection-site reactions |
Urticaria 1 |
1
|
|
A. Injection-site reactions |
Urticaria 1 |
1
|
|
B. Allergic reactions |
Rash 130 |
130
|
|
B. Allergic reactions |
Urticaria 89 |
89
|
|
B. Allergic reactions |
Pruritus 60 |
60
|
|
B. Allergic reactions |
Erythema 47 |
47
|
|
B. Allergic reactions |
Swelling face 42 |
42
|
|
B. Allergic reactions |
Anaphylactic reaction 41 |
41
|
|
B. Allergic reactions |
Dyspnoea 33 |
33
|
|
B. Allergic reactions |
Rash generalised 31 |
31
|
|
B. Allergic reactions |
Rash pruritic 31 |
31
|
|
B. Allergic reactions |
Oedema peripheral 29 |
29
|
|
B. Allergic reactions |
Lip swelling 26 |
26
|
|
B. Allergic reactions |
Rash macular 24 |
24
|
|
B. Allergic reactions |
Dizziness 23 |
23
|
|
B. Allergic reactions |
Hypersensitivity 22 |
22
|
|
B. Allergic reactions |
Eye swelling 18 |
18
|
|
B. Allergic reactions |
Paraesthesia oral 17 |
17
|
|
B. Allergic reactions |
Malaise 15 |
15
|
|
B. Allergic reactions |
Throat tightness 14 |
14
|
|
B. Allergic reactions |
Rash 13 |
13
|
|
B. Allergic reactions |
Swollen tongue 13 |
13
|
|
B. Allergic reactions |
Chest discomfort 11 |
11
|
|
B. Allergic reactions |
Rash erythematous 11 |
11
|
|
B. Allergic reactions |
Feeling hot 9 |
9
|
|
B. Allergic reactions |
Flushing 9 |
9
|
|
B. Allergic reactions |
Pruritus generalised 9 |
9
|
|
B. Allergic reactions |
Dermatitis allergic 8 |
8
|
|
B. Allergic reactions |
Pallor 8 |
8
|
|
B. Allergic reactions |
Pharyngeal oedema 8 |
8
|
|
B. Allergic reactions |
Urticaria 8 |
8
|
|
B. Allergic reactions |
Fatigue 7 |
7
|
|
B. Allergic reactions |
Oropharyngeal pain 7 |
7
|
|
B. Allergic reactions |
Paraesthesia 7 |
7
|
|
B. Allergic reactions |
Angioedema 6 |
6
|
|
B. Allergic reactions |
Dysphagia 6 |
6
|
|
B. Allergic reactions |
Headache 6 |
6
|
|
B. Allergic reactions |
Inflammation 6 |
6
|
|
B. Allergic reactions |
Pyrexia 6 |
6
|
|
B. Allergic reactions |
Throat irritation 6 |
6
|
|
B. Allergic reactions |
Blister 5 |
5
|
|
B. Allergic reactions |
Dyspnoea 5 |
5
|
|
B. Allergic reactions |
Hyperventilation 5 |
5
|
|
B. Allergic reactions |
Hypoaesthesia oral 5 |
5
|
|
B. Allergic reactions |
Vomiting 5 |
5
|
|
B. Allergic reactions |
Wheezing 5 |
5
|
|
B. Allergic reactions |
Anaphylactic shock 4 |
4
|
|
B. Allergic reactions |
Eyelid oedema 4 |
4
|
|
B. Allergic reactions |
Hypersensitivity 4 |
4
|
|
B. Allergic reactions |
Hypoaesthesia 4 |
4
|
|
B. Allergic reactions |
Local swelling 4 |
4
|
|
B. Allergic reactions |
Nausea 4 |
4
|
|
B. Allergic reactions |
Pain in extremity 4 |
4
|
|
B. Allergic reactions |
Dermatitis allergic 3 |
3
|
|
B. Allergic reactions |
Erythema 3 |
3
|
|
B. Allergic reactions |
Eye pruritus 3 |
3
|
|
B. Allergic reactions |
Eyelid oedema 3 |
3
|
|
B. Allergic reactions |
Hyperhidrosis 3 |
3
|
|
B. Allergic reactions |
Laryngeal oedema 3 |
3
|
|
B. Allergic reactions |
Limb discomfort 3 |
3
|
|
B. Allergic reactions |
Nasopharyngitis 3 |
3
|
|
B. Allergic reactions |
Ocular hyperaemia 3 |
3
|
|
B. Allergic reactions |
Pain 3 |
3
|
|
B. Allergic reactions |
Petechiae 3 |
3
|
|
B. Allergic reactions |
Rash erythematous 3 |
3
|
|
B. Allergic reactions |
Rash macular 3 |
3
|
|
B. Allergic reactions |
Rash maculo-papular 3 |
3
|
|
B. Allergic reactions |
Rash pruritic 3 |
3
|
|
B. Allergic reactions |
Skin irritation 3 |
3
|
|
B. Allergic reactions |
Skin reaction 3 |
3
|
|
B. Allergic reactions |
Somnolence 3 |
3
|
|
B. Allergic reactions |
Swelling 3 |
3
|
|
B. Allergic reactions |
Vision blurred 3 |
3
|
|
B. Allergic reactions |
Abdominal pain 2 |
2
|
|
B. Allergic reactions |
Abdominal pain upper 2 |
2
|
|
B. Allergic reactions |
Anaphylactic reaction 2 |
2
|
|
B. Allergic reactions |
Blister 2 |
2
|
|
B. Allergic reactions |
Body temperature increased 2 |
2
|
|
B. Allergic reactions |
Cold sweat 2 |
2
|
|
B. Allergic reactions |
Dermatitis contact 2 |
2
|
|
B. Allergic reactions |
Dizziness 2 |
2
|
|
B. Allergic reactions |
Face oedema 2 |
2
|
|
B. Allergic reactions |
Feeling cold 2 |
2
|
|
B. Allergic reactions |
Heart rate increased 2 |
2
|
|
B. Allergic reactions |
Heart rate irregular 2 |
2
|
|
B. Allergic reactions |
Heat rash 2 |
2
|
|
B. Allergic reactions |
Lip swelling 2 |
2
|
|
B. Allergic reactions |
Peripheral coldness 2 |
2
|
|
B. Allergic reactions |
Pharyngeal oedema 2 |
2
|
|
B. Allergic reactions |
Pruritus 2 |
2
|
|
B. Allergic reactions |
Rash generalised 2 |
2
|
|
B. Allergic reactions |
Skin discolouration 2 |
2
|
|
B. Allergic reactions |
Skin disorder 2 |
2
|
|
B. Allergic reactions |
Swollen tongue 2 |
2
|
|
B. Allergic reactions |
Tachycardia 2 |
2
|
|
B. Allergic reactions |
Type i hypersensitivity 2 |
2
|
|
B. Allergic reactions |
Anaphylactoid reaction 1 |
1
|
|
B. Allergic reactions |
Asthenia 1 |
1
|
|
B. Allergic reactions |
Asthenopia 1 |
1
|
|
B. Allergic reactions |
Asthma 1 |
1
|
|
B. Allergic reactions |
Back pain 1 |
1
|
|
B. Allergic reactions |
Breath sounds abnormal 1 |
1
|
|
B. Allergic reactions |
Bronchospasm 1 |
1
|
|
B. Allergic reactions |
Chest pain 1 |
1
|
|
B. Allergic reactions |
Chills 1 |
1
|
|
B. Allergic reactions |
Condition aggravated 1 |
1
|
|
B. Allergic reactions |
Confusional state 1 |
1
|
|
B. Allergic reactions |
Conjunctival hyperaemia 1 |
1
|
|
B. Allergic reactions |
Contusion 1 |
1
|
|
B. Allergic reactions |
Convulsion 1 |
1
|
|
B. Allergic reactions |
Cough 1 |
1
|
|
B. Allergic reactions |
Dermatitis 1 |
1
|
|
B. Allergic reactions |
Dry throat 1 |
1
|
|
B. Allergic reactions |
Dysphagia 1 |
1
|
|
B. Allergic reactions |
Eczema 1 |
1
|
|
B. Allergic reactions |
Eczema 1 |
1
|
|
B. Allergic reactions |
Eyelid disorder 1 |
1
|
|
B. Allergic reactions |
Eyes sunken 1 |
1
|
|
B. Allergic reactions |
Fatigue 1 |
1
|
|
B. Allergic reactions |
Feeling abnormal 1 |
1
|
|
B. Allergic reactions |
Feeling hot 1 |
1
|
|
B. Allergic reactions |
Feeling jittery 1 |
1
|
|
B. Allergic reactions |
Generalised erythema 1 |
1
|
|
B. Allergic reactions |
Gingival swelling 1 |
1
|
|
B. Allergic reactions |
Headache 1 |
1
|
|
B. Allergic reactions |
Hypersomnia 1 |
1
|
|
B. Allergic reactions |
Hypertension 1 |
1
|
|
B. Allergic reactions |
Hypoventilation 1 |
1
|
|
B. Allergic reactions |
Increased bronchial secretion 1 |
1
|
|
B. Allergic reactions |
Infusion site swelling 1 |
1
|
|
B. Allergic reactions |
Laryngeal oedema 1 |
1
|
|
B. Allergic reactions |
Lethargy 1 |
1
|
|
B. Allergic reactions |
Lip blister 1 |
1
|
|
B. Allergic reactions |
Lip ulceration 1 |
1
|
|
B. Allergic reactions |
Local reaction 1 |
1
|
|
B. Allergic reactions |
Loss of consciousness 1 |
1
|
|
B. Allergic reactions |
Migraine 1 |
1
|
|
B. Allergic reactions |
Muscle tightness 1 |
1
|
|
B. Allergic reactions |
Musculoskeletal stiffness 1 |
1
|
|
B. Allergic reactions |
Myalgia 1 |
1
|
|
B. Allergic reactions |
Mydriasis 1 |
1
|
|
B. Allergic reactions |
Nausea 1 |
1
|
|
B. Allergic reactions |
Neck pain 1 |
1
|
|
B. Allergic reactions |
Oedema mouth 1 |
1
|
|
B. Allergic reactions |
Oedema mouth 1 |
1
|
|
B. Allergic reactions |
Oesophageal discomfort 1 |
1
|
|
B. Allergic reactions |
Oral discomfort 1 |
1
|
|
B. Allergic reactions |
Oral pain 1 |
1
|
|
B. Allergic reactions |
Palpitations 1 |
1
|
|
B. Allergic reactions |
Panic reaction 1 |
1
|
|
B. Allergic reactions |
Paraesthesia oral 1 |
1
|
|
B. Allergic reactions |
Periorbital oedema 1 |
1
|
|
B. Allergic reactions |
Photophobia 1 |
1
|
|
B. Allergic reactions |
Piloerection 1 |
1
|
|
B. Allergic reactions |
Pulse absent 1 |
1
|
|
B. Allergic reactions |
Purpura 1 |
1
|
|
B. Allergic reactions |
Pyrexia 1 |
1
|
|
B. Allergic reactions |
Rash follicular 1 |
1
|
|
B. Allergic reactions |
Rash papular 1 |
1
|
|
B. Allergic reactions |
Respiratory rate increased 1 |
1
|
|
B. Allergic reactions |
Sensation of foreign body 1 |
1
|
|
B. Allergic reactions |
Sneezing 1 |
1
|
|
B. Allergic reactions |
Somnolence 1 |
1
|
|
B. Allergic reactions |
Speech disorder 1 |
1
|
|
B. Allergic reactions |
Stridor 1 |
1
|
|
B. Allergic reactions |
Swelling 1 |
1
|
|
B. Allergic reactions |
Swelling face 1 |
1
|
|
B. Allergic reactions |
Syncope 1 |
1
|
|
B. Allergic reactions |
Systemic lupus erythematosus rash 1 |
1
|
|
B. Allergic reactions |
Tenderness 1 |
1
|
|
B. Allergic reactions |
Thirst 1 |
1
|
|
B. Allergic reactions |
Throat irritation 1 |
1
|
|
B. Allergic reactions |
Throat tightness 1 |
1
|
|
B. Allergic reactions |
Tremor 1 |
1
|
|
B. Allergic reactions |
Type IV hypersensitivity reaction 1 |
1
|
|
B. Allergic reactions |
Urticaria pigmentosa 1 |
1
|
|
B. Allergic reactions |
Visual impairment 1 |
1
|
|
B. Allergic reactions |
Vomiting 1 |
1
|
|
C. ‘Psychogenic’ events |
Dizziness 327 |
327
|
|
C. ‘Psychogenic’ events |
Syncope 296 |
296
|
|
C. ‘Psychogenic’ events |
Nausea 151 |
151
|
|
C. ‘Psychogenic’ events |
Headache 109 |
109
|
|
C. ‘Psychogenic’ events |
Pallor 108 |
108
|
|
C. ‘Psychogenic’ events |
Vomiting 77 |
77
|
|
C. ‘Psychogenic’ events |
Malaise 74 |
74
|
|
C. ‘Psychogenic’ events |
Tremor 61 |
61
|
|
C. ‘Psychogenic’ events |
Vision blurred 46 |
46
|
|
C. ‘Psychogenic’ events |
Feeling hot 45 |
45
|
|
C. ‘Psychogenic’ events |
Flushing 40 |
40
|
|
C. ‘Psychogenic’ events |
Cold sweat 35 |
35
|
|
C. ‘Psychogenic’ events |
Syncope 27 |
27
|
|
C. ‘Psychogenic’ events |
Hyperhidrosis 25 |
25
|
|
C. ‘Psychogenic’ events |
Presyncope 23 |
23
|
|
C. ‘Psychogenic’ events |
Hyperventilation 21 |
21
|
|
C. ‘Psychogenic’ events |
Loss of consciousness 19 |
19
|
|
C. ‘Psychogenic’ events |
Dyspnoea 18 |
18
|
|
C. ‘Psychogenic’ events |
Paraesthesia 18 |
18
|
|
C. ‘Psychogenic’ events |
Chills 17 |
17
|
|
C. ‘Psychogenic’ events |
Convulsion 17 |
17
|
|
C. ‘Psychogenic’ events |
Pyrexia 16 |
16
|
|
C. ‘Psychogenic’ events |
Somnolence 16 |
16
|
|
C. ‘Psychogenic’ events |
Dizziness 15 |
15
|
|
C. ‘Psychogenic’ events |
Fatigue 15 |
15
|
|
C. ‘Psychogenic’ events |
Heart rate increased 14 |
14
|
|
C. ‘Psychogenic’ events |
Unresponsive to stimuli 14 |
14
|
|
C. ‘Psychogenic’ events |
Muscle twitching 13 |
13
|
|
C. ‘Psychogenic’ events |
Rash 13 |
13
|
|
C. ‘Psychogenic’ events |
Asthenia 12 |
12
|
|
C. ‘Psychogenic’ events |
Feeling cold 12 |
12
|
|
C. ‘Psychogenic’ events |
Hypoaesthesia 12 |
12
|
|
C. ‘Psychogenic’ events |
Panic attack 12 |
12
|
|
C. ‘Psychogenic’ events |
Chest discomfort 11 |
11
|
|
C. ‘Psychogenic’ events |
Dyskinesia 11 |
11
|
|
C. ‘Psychogenic’ events |
Eye rolling 11 |
11
|
|
C. ‘Psychogenic’ events |
Tachycardia 11 |
11
|
|
C. ‘Psychogenic’ events |
Tearfulness 11 |
11
|
|
C. ‘Psychogenic’ events |
Nervousness 10 |
10
|
|
C. ‘Psychogenic’ events |
Erythema 9 |
9
|
|
C. ‘Psychogenic’ events |
Headache 9 |
9
|
|
C. ‘Psychogenic’ events |
Rash macular 9 |
9
|
|
C. ‘Psychogenic’ events |
Abdominal pain 8 |
8
|
|
C. ‘Psychogenic’ events |
Chest pain 8 |
8
|
|
C. ‘Psychogenic’ events |
Peripheral coldness 8 |
8
|
|
C. ‘Psychogenic’ events |
Abdominal pain upper 7 |
7
|
|
C. ‘Psychogenic’ events |
Anxiety 7 |
7
|
|
C. ‘Psychogenic’ events |
Fall 7 |
7
|
|
C. ‘Psychogenic’ events |
Hypotension 7 |
7
|
|
C. ‘Psychogenic’ events |
Lethargy 7 |
7
|
|
C. ‘Psychogenic’ events |
Muscular weakness 7 |
7
|
|
C. ‘Psychogenic’ events |
Photophobia 7 |
7
|
|
C. ‘Psychogenic’ events |
Visual impairment 7 |
7
|
|
C. ‘Psychogenic’ events |
Confusional state 6 |
6
|
|
C. ‘Psychogenic’ events |
Deafness 6 |
6
|
|
C. ‘Psychogenic’ events |
Feeling of body temperature change 6 |
6
|
|
C. ‘Psychogenic’ events |
Muscle rigidity 6 |
6
|
|
C. ‘Psychogenic’ events |
Musculoskeletal stiffness 6 |
6
|
|
C. ‘Psychogenic’ events |
Mydriasis 6 |
6
|
|
C. ‘Psychogenic’ events |
Nasopharyngitis 6 |
6
|
|
C. ‘Psychogenic’ events |
Throat tightness 6 |
6
|
|
C. ‘Psychogenic’ events |
Dizziness postural 5 |
5
|
|
C. ‘Psychogenic’ events |
Dysgeusia 5 |
5
|
|
C. ‘Psychogenic’ events |
Feeling abnormal 5 |
5
|
|
C. ‘Psychogenic’ events |
Pallor 5 |
5
|
|
C. ‘Psychogenic’ events |
Skin discolouration 5 |
5
|
|
C. ‘Psychogenic’ events |
Urticaria 5 |
5
|
|
C. ‘Psychogenic’ events |
Abdominal discomfort 4 |
4
|
|
C. ‘Psychogenic’ events |
Blindness transient 4 |
4
|
|
C. ‘Psychogenic’ events |
Body temperature increased 4 |
4
|
|
C. ‘Psychogenic’ events |
Decreased appetite 4 |
4
|
|
C. ‘Psychogenic’ events |
Hot flush 4 |
4
|
|
C. ‘Psychogenic’ events |
Migraine 4 |
4
|
|
C. ‘Psychogenic’ events |
Muscle spasms 4 |
4
|
|
C. ‘Psychogenic’ events |
Pulse abnormal 4 |
4
|
|
C. ‘Psychogenic’ events |
Respiratory rate increased 4 |
4
|
|
C. ‘Psychogenic’ events |
Tinnitus 4 |
4
|
|
C. ‘Psychogenic’ events |
Urinary incontinence 4 |
4
|
|
C. ‘Psychogenic’ events |
Vomiting 4 |
4
|
|
C. ‘Psychogenic’ events |
Abasia 3 |
3
|
|
C. ‘Psychogenic’ events |
Agitation 3 |
3
|
|
C. ‘Psychogenic’ events |
Balance disorder 3 |
3
|
|
C. ‘Psychogenic’ events |
Blindness 3 |
3
|
|
C. ‘Psychogenic’ events |
Blood pressure decreased 3 |
3
|
|
C. ‘Psychogenic’ events |
Cyanosis 3 |
3
|
|
C. ‘Psychogenic’ events |
Disorientation 3 |
3
|
|
C. ‘Psychogenic’ events |
Disturbance in attention 3 |
3
|
|
C. ‘Psychogenic’ events |
Dyspnoea 3 |
3
|
|
C. ‘Psychogenic’ events |
Dysstasia 3 |
3
|
|
C. ‘Psychogenic’ events |
Emotional disorder 3 |
3
|
|
C. ‘Psychogenic’ events |
Feeling drunk 3 |
3
|
|
C. ‘Psychogenic’ events |
Hearing impaired 3 |
3
|
|
C. ‘Psychogenic’ events |
Heart rate irregular 3 |
3
|
|
C. ‘Psychogenic’ events |
Hypoventilation 3 |
3
|
|
C. ‘Psychogenic’ events |
Nausea 3 |
3
|
|
C. ‘Psychogenic’ events |
Pain 3 |
3
|
|
C. ‘Psychogenic’ events |
Pain in extremity 3 |
3
|
|
C. ‘Psychogenic’ events |
Panic reaction 3 |
3
|
|
C. ‘Psychogenic’ events |
Rash 3 |
3
|
|
C. ‘Psychogenic’ events |
Sensory loss 3 |
3
|
|
C. ‘Psychogenic’ events |
Somnolence 3 |
3
|
|
C. ‘Psychogenic’ events |
Throat irritation 3 |
3
|
|
C. ‘Psychogenic’ events |
Vertigo 3 |
3
|
|
C. ‘Psychogenic’ events |
Amnesia 2 |
2
|
|
C. ‘Psychogenic’ events |
Blood pressure increased 2 |
2
|
|
C. ‘Psychogenic’ events |
Body temperature decreased 2 |
2
|
|
C. ‘Psychogenic’ events |
Bradycardia 2 |
2
|
|
C. ‘Psychogenic’ events |
Circulatory collapse 2 |
2
|
|
C. ‘Psychogenic’ events |
Colour blindness acquired 2 |
2
|
|
C. ‘Psychogenic’ events |
Consciousness fluctuating 2 |
2
|
|
C. ‘Psychogenic’ events |
Diplopia 2 |
2
|
|
C. ‘Psychogenic’ events |
Dry mouth 2 |
2
|
|
C. ‘Psychogenic’ events |
Dry throat 2 |
2
|
|
C. ‘Psychogenic’ events |
Dysarthria 2 |
2
|
|
C. ‘Psychogenic’ events |
Dysphagia 2 |
2
|
|
C. ‘Psychogenic’ events |
Emotional distress 2 |
2
|
|
C. ‘Psychogenic’ events |
Heart rate decreased 2 |
2
|
|
C. ‘Psychogenic’ events |
Heart rate increased 2 |
2
|
|
C. ‘Psychogenic’ events |
Hypertension 2 |
2
|
|
C. ‘Psychogenic’ events |
Hyperventilation 2 |
2
|
|
C. ‘Psychogenic’ events |
Hypoacusis 2 |
2
|
|
C. ‘Psychogenic’ events |
Malaise 2 |
2
|
|
C. ‘Psychogenic’ events |
Muscular weakness 2 |
2
|
|
C. ‘Psychogenic’ events |
Myalgia 2 |
2
|
|
C. ‘Psychogenic’ events |
Neck pain 2 |
2
|
|
C. ‘Psychogenic’ events |
Oropharyngeal pain 2 |
2
|
|
C. ‘Psychogenic’ events |
Paraesthesia oral 2 |
2
|
|
C. ‘Psychogenic’ events |
Presyncope 2 |
2
|
|
C. ‘Psychogenic’ events |
Procedural dizziness 2 |
2
|
|
C. ‘Psychogenic’ events |
Pruritus 2 |
2
|
|
C. ‘Psychogenic’ events |
Pulse pressure decreased 2 |
2
|
|
C. ‘Psychogenic’ events |
Pupil fixed 2 |
2
|
|
C. ‘Psychogenic’ events |
Rash generalised 2 |
2
|
|
C. ‘Psychogenic’ events |
Retching 2 |
2
|
|
C. ‘Psychogenic’ events |
Salivary hypersecretion 2 |
2
|
|
C. ‘Psychogenic’ events |
Shock 2 |
2
|
|
C. ‘Psychogenic’ events |
Vision blurred 2 |
2
|
|
C. ‘Psychogenic’ events |
Abdominal discomfort 1 |
1
|
|
C. ‘Psychogenic’ events |
Abdominal distension 1 |
1
|
|
C. ‘Psychogenic’ events |
Abdominal pain 1 |
1
|
|
C. ‘Psychogenic’ events |
Abnormal behaviour 1 |
1
|
|
C. ‘Psychogenic’ events |
Altered state of consciousness 1 |
1
|
|
C. ‘Psychogenic’ events |
Aphasia 1 |
1
|
|
C. ‘Psychogenic’ events |
Asthenia 1 |
1
|
|
C. ‘Psychogenic’ events |
Asthma 1 |
1
|
|
C. ‘Psychogenic’ events |
Back pain 1 |
1
|
|
C. ‘Psychogenic’ events |
Blindness transient 1 |
1
|
|
C. ‘Psychogenic’ events |
Blood pressure increased 1 |
1
|
|
C. ‘Psychogenic’ events |
Blood pressure systolic decreased 1 |
1
|
|
C. ‘Psychogenic’ events |
Body temperature decreased 1 |
1
|
|
C. ‘Psychogenic’ events |
Bruxism 1 |
1
|
|
C. ‘Psychogenic’ events |
Burning sensation 1 |
1
|
|
C. ‘Psychogenic’ events |
Chills 1 |
1
|
|
C. ‘Psychogenic’ events |
Condition aggravated 1 |
1
|
|
C. ‘Psychogenic’ events |
Convulsion 1 |
1
|
|
C. ‘Psychogenic’ events |
Cough 1 |
1
|
|
C. ‘Psychogenic’ events |
Deafness transitory 1 |
1
|
|
C. ‘Psychogenic’ events |
Depressed level of consciousness 1 |
1
|
|
C. ‘Psychogenic’ events |
Discomfort 1 |
1
|
|
C. ‘Psychogenic’ events |
Dissociation 1 |
1
|
|
C. ‘Psychogenic’ events |
Disturbance in attention 1 |
1
|
|
C. ‘Psychogenic’ events |
Dry mouth 1 |
1
|
|
C. ‘Psychogenic’ events |
Ear discomfort 1 |
1
|
|
C. ‘Psychogenic’ events |
Ear pain 1 |
1
|
|
C. ‘Psychogenic’ events |
Epistaxis 1 |
1
|
|
C. ‘Psychogenic’ events |
Eye pain 1 |
1
|
|
C. ‘Psychogenic’ events |
Eyelid oedema 1 |
1
|
|
C. ‘Psychogenic’ events |
Face injury 1 |
1
|
|
C. ‘Psychogenic’ events |
Facial spasm 1 |
1
|
|
C. ‘Psychogenic’ events |
Fatigue 1 |
1
|
|
C. ‘Psychogenic’ events |
Fear 1 |
1
|
|
C. ‘Psychogenic’ events |
Feeling of despair 1 |
1
|
|
C. ‘Psychogenic’ events |
Foaming at mouth 1 |
1
|
|
C. ‘Psychogenic’ events |
Gait disturbance 1 |
1
|
|
C. ‘Psychogenic’ events |
Grand mal convulsion 1 |
1
|
|
C. ‘Psychogenic’ events |
Grip strength decreased 1 |
1
|
|
C. ‘Psychogenic’ events |
Head banging 1 |
1
|
|
C. ‘Psychogenic’ events |
Head discomfort 1 |
1
|
|
C. ‘Psychogenic’ events |
Heart rate irregular 1 |
1
|
|
C. ‘Psychogenic’ events |
Heat rash 1 |
1
|
|
C. ‘Psychogenic’ events |
Hemiparesis 1 |
1
|
|
C. ‘Psychogenic’ events |
Hot flush 1 |
1
|
|
C. ‘Psychogenic’ events |
Hyperhidrosis 1 |
1
|
|
C. ‘Psychogenic’ events |
Hypersomnia 1 |
1
|
|
C. ‘Psychogenic’ events |
Hypoaesthesia 1 |
1
|
|
C. ‘Psychogenic’ events |
Hypoaesthesia facial 1 |
1
|
|
C. ‘Psychogenic’ events |
Hypokinesia 1 |
1
|
|
C. ‘Psychogenic’ events |
Hypotonia 1 |
1
|
|
C. ‘Psychogenic’ events |
Incontinence 1 |
1
|
|
C. ‘Psychogenic’ events |
Lip swelling 1 |
1
|
|
C. ‘Psychogenic’ events |
Livedo reticularis 1 |
1
|
|
C. ‘Psychogenic’ events |
Migraine 1 |
1
|
|
C. ‘Psychogenic’ events |
Muscle contracture 1 |
1
|
|
C. ‘Psychogenic’ events |
Myoclonus 1 |
1
|
|
C. ‘Psychogenic’ events |
Nervous system disorder 1 |
1
|
|
C. ‘Psychogenic’ events |
Oral discomfort 1 |
1
|
|
C. ‘Psychogenic’ events |
Palpitations 1 |
1
|
|
C. ‘Psychogenic’ events |
Paraesthesia 1 |
1
|
|
C. ‘Psychogenic’ events |
Peripheral circulatory failure 1 |
1
|
|
C. ‘Psychogenic’ events |
Pharyngeal oedema 1 |
1
|
|
C. ‘Psychogenic’ events |
Photophobia 1 |
1
|
|
C. ‘Psychogenic’ events |
Poor peripheral circulation 1 |
1
|
|
C. ‘Psychogenic’ events |
Pruritus 1 |
1
|
|
C. ‘Psychogenic’ events |
Psychomotor hyperactivity 1 |
1
|
|
C. ‘Psychogenic’ events |
Pyrexia 1 |
1
|
|
C. ‘Psychogenic’ events |
Respiratory arrest 1 |
1
|
|
C. ‘Psychogenic’ events |
Respiratory rate decreased 1 |
1
|
|
C. ‘Psychogenic’ events |
Seizure anoxic 1 |
1
|
|
C. ‘Psychogenic’ events |
Sensation of heaviness 1 |
1
|
|
C. ‘Psychogenic’ events |
Sensory loss 1 |
1
|
|
C. ‘Psychogenic’ events |
Sinus tachycardia 1 |
1
|
|
C. ‘Psychogenic’ events |
Sleep attacks 1 |
1
|
|
C. ‘Psychogenic’ events |
Sudden onset of sleep 1 |
1
|
|
C. ‘Psychogenic’ events |
Tachypnoea 1 |
1
|
|
C. ‘Psychogenic’ events |
Tremor 1 |
1
|
|
C. ‘Psychogenic’ events |
Urticaria 1 |
1
|
|
C. ‘Psychogenic’ events |
Visual impairment 1 |
1
|
|
D. ‘Other recognised’ reactions |
Nausea 631 |
631
|
|
D. ‘Other recognised’ reactions |
Headache 629 |
629
|
|
D. ‘Other recognised’ reactions |
Dizziness 625 |
625
|
|
D. ‘Other recognised’ reactions |
Vomiting 260 |
260
|
|
D. ‘Other recognised’ reactions |
Malaise 220 |
220
|
|
D. ‘Other recognised’ reactions |
Fatigue 216 |
216
|
|
D. ‘Other recognised’ reactions |
Pyrexia 175 |
175
|
|
D. ‘Other recognised’ reactions |
Abdominal pain 69 |
69
|
|
D. ‘Other recognised’ reactions |
Diarrhoea 55 |
55
|
|
D. ‘Other recognised’ reactions |
Abdominal pain upper 54 |
54
|
|
D. ‘Other recognised’ reactions |
Myalgia 49 |
49
|
|
D. ‘Other recognised’ reactions |
Lethargy 48 |
48
|
|
D. ‘Other recognised’ reactions |
Feeling hot 43 |
43
|
|
D. ‘Other recognised’ reactions |
Body temperature increased 36 |
36
|
|
D. ‘Other recognised’ reactions |
Pain 34 |
34
|
|
D. ‘Other recognised’ reactions |
Headache 30 |
30
|
|
D. ‘Other recognised’ reactions |
Influenza like illness 28 |
28
|
|
D. ‘Other recognised’ reactions |
Nausea 28 |
28
|
|
D. ‘Other recognised’ reactions |
Oropharyngeal pain 28 |
28
|
|
D. ‘Other recognised’ reactions |
Arthralgia 25 |
25
|
|
D. ‘Other recognised’ reactions |
Malaise 25 |
25
|
|
D. ‘Other recognised’ reactions |
Pyrexia 24 |
24
|
|
D. ‘Other recognised’ reactions |
Pallor 22 |
22
|
|
D. ‘Other recognised’ reactions |
Somnolence 22 |
22
|
|
D. ‘Other recognised’ reactions |
Asthenia 21 |
21
|
|
D. ‘Other recognised’ reactions |
Chills 21 |
21
|
|
D. ‘Other recognised’ reactions |
Pain in extremity 21 |
21
|
|
D. ‘Other recognised’ reactions |
Rash 21 |
21
|
| Musculoskeletal and connective tissue disorders |
D. ‘Other recognised’ reactions |
Arthralgia 20 |
20
|
|
D. ‘Other recognised’ reactions |
Lymphadenopathy 18 |
18
|
|
D. ‘Other recognised’ reactions |
Vomiting 16 |
16
|
|
D. ‘Other recognised’ reactions |
Abdominal discomfort 15 |
15
|
|
D. ‘Other recognised’ reactions |
Dizziness 15 |
15
|
|
D. ‘Other recognised’ reactions |
Flushing 14 |
14
|
|
D. ‘Other recognised’ reactions |
Paraesthesia 14 |
14
|
|
D. ‘Other recognised’ reactions |
Fatigue 12 |
12
|
|
D. ‘Other recognised’ reactions |
Tremor 12 |
12
|
|
D. ‘Other recognised’ reactions |
Pruritus 11 |
11
|
|
D. ‘Other recognised’ reactions |
Decreased appetite 10 |
10
|
|
D. ‘Other recognised’ reactions |
Abdominal pain 8 |
8
|
|
D. ‘Other recognised’ reactions |
Neck pain 8 |
8
|
|
D. ‘Other recognised’ reactions |
Feeling cold 7 |
7
|
|
D. ‘Other recognised’ reactions |
Back pain 6 |
6
|
|
D. ‘Other recognised’ reactions |
Cough 6 |
6
|
|
D. ‘Other recognised’ reactions |
Hyperhidrosis 6 |
6
|
|
D. ‘Other recognised’ reactions |
Hypoaesthesia 6 |
6
|
|
D. ‘Other recognised’ reactions |
Lethargy 6 |
6
|
|
D. ‘Other recognised’ reactions |
Musculoskeletal stiffness 6 |
6
|
|
D. ‘Other recognised’ reactions |
Nasopharyngitis 6 |
6
|
|
D. ‘Other recognised’ reactions |
Abdominal pain upper 5 |
5
|
|
D. ‘Other recognised’ reactions |
Asthenia 4 |
4
|
|
D. ‘Other recognised’ reactions |
Body temperature increased 4 |
4
|
|
D. ‘Other recognised’ reactions |
Erythema 4 |
4
|
|
D. ‘Other recognised’ reactions |
Feeling of body temperature change 4 |
4
|
|
D. ‘Other recognised’ reactions |
Migraine 4 |
4
|
|
D. ‘Other recognised’ reactions |
Myalgia 4 |
4
|
|
D. ‘Other recognised’ reactions |
Nervousness 4 |
4
|
|
D. ‘Other recognised’ reactions |
Back pain 3 |
3
|
|
D. ‘Other recognised’ reactions |
Decreased appetite 3 |
3
|
|
D. ‘Other recognised’ reactions |
Diarrhoea 3 |
3
|
|
D. ‘Other recognised’ reactions |
Lower respiratory tract infection 3 |
3
|
|
D. ‘Other recognised’ reactions |
Muscle fatigue 3 |
3
|
|
D. ‘Other recognised’ reactions |
Muscular weakness 3 |
3
|
|
D. ‘Other recognised’ reactions |
Rash generalised 3 |
3
|
|
D. ‘Other recognised’ reactions |
Somnolence 3 |
3
|
|
D. ‘Other recognised’ reactions |
Cold sweat 2 |
2
|
|
D. ‘Other recognised’ reactions |
Dizziness postural 2 |
2
|
|
D. ‘Other recognised’ reactions |
Feeling abnormal 2 |
2
|
|
D. ‘Other recognised’ reactions |
Gait disturbance 2 |
2
|
|
D. ‘Other recognised’ reactions |
Head discomfort 2 |
2
|
|
D. ‘Other recognised’ reactions |
Hot flush 2 |
2
|
|
D. ‘Other recognised’ reactions |
Influenza like illness 2 |
2
|
|
D. ‘Other recognised’ reactions |
Joint swelling 2 |
2
|
|
D. ‘Other recognised’ reactions |
Limb discomfort 2 |
2
|
|
D. ‘Other recognised’ reactions |
Listless 2 |
2
|
|
D. ‘Other recognised’ reactions |
Local reaction 2 |
2
|
|
D. ‘Other recognised’ reactions |
Musculoskeletal stiffness 2 |
2
|
|
D. ‘Other recognised’ reactions |
Nasal congestion 2 |
2
|
|
D. ‘Other recognised’ reactions |
Oropharyngeal pain 2 |
2
|
|
D. ‘Other recognised’ reactions |
Pain 2 |
2
|
|
D. ‘Other recognised’ reactions |
Pruritus generalised 2 |
2
|
|
D. ‘Other recognised’ reactions |
Rash macular 2 |
2
|
|
D. ‘Other recognised’ reactions |
Skin warm 2 |
2
|
|
D. ‘Other recognised’ reactions |
Throat irritation 2 |
2
|
|
D. ‘Other recognised’ reactions |
Abdominal pain lower 1 |
1
|
|
D. ‘Other recognised’ reactions |
Abdominal pain lower 1 |
1
|
|
D. ‘Other recognised’ reactions |
Arthralgia 1 |
1
|
|
D. ‘Other recognised’ reactions |
Axillary mass 1 |
1
|
|
D. ‘Other recognised’ reactions |
Bedridden 1 |
1
|
|
D. ‘Other recognised’ reactions |
Body temperature 1 |
1
|
|
D. ‘Other recognised’ reactions |
Body temperature fluctuation 1 |
1
|
|
D. ‘Other recognised’ reactions |
Body temperature fluctuation 1 |
1
|
|
D. ‘Other recognised’ reactions |
Cough 1 |
1
|
|
D. ‘Other recognised’ reactions |
Dyspnoea 1 |
1
|
|
D. ‘Other recognised’ reactions |
Feeling of body temperature change 1 |
1
|
|
D. ‘Other recognised’ reactions |
Gastrointestinal disorder 1 |
1
|
|
D. ‘Other recognised’ reactions |
Generalised erythema 1 |
1
|
|
D. ‘Other recognised’ reactions |
Groin pain 1 |
1
|
|
D. ‘Other recognised’ reactions |
Hot flush 1 |
1
|
|
D. ‘Other recognised’ reactions |
Hypoaesthesia 1 |
1
|
|
D. ‘Other recognised’ reactions |
Hypotension 1 |
1
|
|
D. ‘Other recognised’ reactions |
Ill-defined disorder 1 |
1
|
|
D. ‘Other recognised’ reactions |
Immunisation reaction 1 |
1
|
|
D. ‘Other recognised’ reactions |
Induration 1 |
1
|
|
D. ‘Other recognised’ reactions |
Insomnia 1 |
1
|
|
D. ‘Other recognised’ reactions |
Limb discomfort 1 |
1
|
|
D. ‘Other recognised’ reactions |
Local reaction 1 |
1
|
|
D. ‘Other recognised’ reactions |
Local swelling 1 |
1
|
|
D. ‘Other recognised’ reactions |
Loss of consciousness 1 |
1
|
|
D. ‘Other recognised’ reactions |
Lymphadenopathy 1 |
1
|
|
D. ‘Other recognised’ reactions |
Mobility decreased 1 |
1
|
|
D. ‘Other recognised’ reactions |
Muscle spasms 1 |
1
|
|
D. ‘Other recognised’ reactions |
Muscle twitching 1 |
1
|
|
D. ‘Other recognised’ reactions |
Musculoskeletal chest pain 1 |
1
|
|
D. ‘Other recognised’ reactions |
Musculoskeletal discomfort 1 |
1
|
|
D. ‘Other recognised’ reactions |
Musculoskeletal discomfort 1 |
1
|
|
D. ‘Other recognised’ reactions |
Musculoskeletal pain 1 |
1
|
|
D. ‘Other recognised’ reactions |
Neck pain 1 |
1
|
|
D. ‘Other recognised’ reactions |
Night sweats 1 |
1
|
|
D. ‘Other recognised’ reactions |
Pain in extremity 1 |
1
|
|
D. ‘Other recognised’ reactions |
Peripheral coldness 1 |
1
|
|
D. ‘Other recognised’ reactions |
Pharyngitis 1 |
1
|
|
D. ‘Other recognised’ reactions |
Rash erythematous 1 |
1
|
|
D. ‘Other recognised’ reactions |
Respiratory disorder 1 |
1
|
|
D. ‘Other recognised’ reactions |
Respiratory tract infection 1 |
1
|
|
D. ‘Other recognised’ reactions |
Restlessness 1 |
1
|
|
D. ‘Other recognised’ reactions |
Rhinorrhoea 1 |
1
|
|
D. ‘Other recognised’ reactions |
Sensation of heaviness 1 |
1
|
|
D. ‘Other recognised’ reactions |
Sudden onset of sleep 1 |
1
|
|
D. ‘Other recognised’ reactions |
Swelling 1 |
1
|
|
D. ‘Other recognised’ reactions |
Swelling face 1 |
1
|
|
D. ‘Other recognised’ reactions |
Syncope 1 |
1
|
|
D. ‘Other recognised’ reactions |
Thirst 1 |
1
|
|
D. ‘Other recognised’ reactions |
Throat tightness 1 |
1
|
|
D. ‘Other recognised’ reactions |
Upper respiratory tract infection 1 |
1
|
|
D. ‘Other recognised’ reactions |
Urticaria 1 |
1
|
|
D. ‘Other recognised’ reactions |
Weight decreased 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Headache 47 |
47
|
| Nervous system disorders |
E. not currently recognised |
Syncope 35 |
35
|
| General disorders and administration site conditions |
E. not currently recognised |
Influenza like illness 32 |
32
|
| Nervous system disorders |
E. not currently recognised |
Dizziness 29 |
29
|
| Nervous system disorders |
E. not currently recognised |
Hypoaesthesia 29 |
29
|
| Nervous system disorders |
E. not currently recognised |
Convulsion 28 |
28
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Pain in extremity 27 |
27
|
| Gastrointestinal disorders |
E. not currently recognised |
Nausea 24 |
24
|
| Nervous system disorders |
E. not currently recognised |
Paraesthesia 20 |
20
|
| Respiratory, thoracic and mediastinal disorders |
E. not currently recognised |
Dyspnoea 19 |
19
|
| Nervous system disorders |
E. not currently recognised |
Lethargy 19 |
19
|
| General disorders and administration site conditions |
E. not currently recognised |
Malaise 19 |
19
|
| Injury, poisoning and procedural complications |
E. not currently recognised |
Drug exposure during pregnancy 18 |
18
|
| General disorders and administration site conditions |
E. not currently recognised |
Fatigue 18 |
18
|
| General disorders and administration site conditions |
E. not currently recognised |
Pyrexia 18 |
18
|
| General disorders and administration site conditions |
E. not currently recognised |
Chest pain 17 |
17
|
| Gastrointestinal disorders |
E. not currently recognised |
Vomiting 17 |
17
|
| Nervous system disorders |
E. not currently recognised |
Migraine 16 |
16
|
| General disorders and administration site conditions |
E. not currently recognised |
Pain 16 |
16
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Back pain 15 |
15
|
| Nervous system disorders |
E. not currently recognised |
Somnolence 14 |
14
|
| Nervous system disorders |
E. not currently recognised |
Tremor 14 |
14
|
| Nervous system disorders |
E. not currently recognised |
Dizziness 12 |
12
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Muscular weakness 12 |
12
|
| Pregnancy, puerperium and perinatal conditions |
E. not currently recognised |
Abortion spontaneous 11 |
11
|
| General disorders and administration site conditions |
E. not currently recognised |
Asthenia 11 |
11
|
| Nervous system disorders |
E. not currently recognised |
Headache 11 |
11
|
| Nervous system disorders |
E. not currently recognised |
Loss of consciousness 11 |
11
|
| Gastrointestinal disorders |
E. not currently recognised |
Abdominal pain 10 |
10
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Myalgia 10 |
10
|
| Respiratory, thoracic and mediastinal disorders |
E. not currently recognised |
Oropharyngeal pain 10 |
10
|
| Reproductive system and breast disorders |
E. not currently recognised |
Amenorrhoea 9 |
9
|
| General disorders and administration site conditions |
E. not currently recognised |
Chest discomfort 9 |
9
|
| Vascular disorders |
E. not currently recognised |
Peripheral coldness 9 |
9
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Alopecia 8 |
8
|
| Respiratory, thoracic and mediastinal disorders |
E. not currently recognised |
Cough 8 |
8
|
| Metabolism and nutrition disorders |
E. not currently recognised |
Decreased appetite 8 |
8
|
| Respiratory, thoracic and mediastinal disorders |
E. not currently recognised |
Epistaxis 8 |
8
|
| General disorders and administration site conditions |
E. not currently recognised |
Fatigue 8 |
8
|
| General disorders and administration site conditions |
E. not currently recognised |
Influenza like illness 8 |
8
|
| Eye disorders |
E. not currently recognised |
Vision blurred 8 |
8
|
| Respiratory, thoracic and mediastinal disorders |
E. not currently recognised |
Asthma 7 |
7
|
| Gastrointestinal disorders |
E. not currently recognised |
Diarrhoea 7 |
7
|
| General disorders and administration site conditions |
E. not currently recognised |
Feeling cold 7 |
7
|
| Nervous system disorders |
E. not currently recognised |
Hypoaesthesia 7 |
7
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Hypoaesthesia facial 7 |
7
|
| Eye disorders |
E. not currently recognised |
Photophobia 7 |
7
|
| Nervous system disorders |
E. not currently recognised |
Syncope 7 |
7
|
| Reproductive system and breast disorders |
E. not currently recognised |
Vaginal haemorrhage 7 |
7
|
| Infections and infestations |
E. not currently recognised |
Viral infection 7 |
7
|
| Eye disorders |
E. not currently recognised |
Vision blurred 7 |
7
|
| Gastrointestinal disorders |
E. not currently recognised |
Abdominal pain 6 |
6
|
| Nervous system disorders |
E. not currently recognised |
Dysarthria 6 |
6
|
| Ear and labyrinth disorders |
E. not currently recognised |
Ear pain 6 |
6
|
| Nervous system disorders |
E. not currently recognised |
Epilepsy 6 |
6
|
| Psychiatric disorders |
E. not currently recognised |
Hallucination 6 |
6
|
| Psychiatric disorders |
E. not currently recognised |
Insomnia 6 |
6
|
| Infections and infestations |
E. not currently recognised |
Lower respiratory tract infection 6 |
6
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Musculoskeletal stiffness 6 |
6
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Neck pain 6 |
6
|
| Cardiac disorders |
E. not currently recognised |
Palpitations 6 |
6
|
| Nervous system disorders |
E. not currently recognised |
Paraesthesia 6 |
6
|
| Infections and infestations |
E. not currently recognised |
Post viral fatigue syndrome 6 |
6
|
| Nervous system disorders |
E. not currently recognised |
Sensory disturbance 6 |
6
|
| Eye disorders |
E. not currently recognised |
Visual impairment 6 |
6
|
| General disorders and administration site conditions |
E. not currently recognised |
Abasia 5 |
5
|
| Nervous system disorders |
E. not currently recognised |
Dyskinesia 5 |
5
|
| Nervous system disorders |
E. not currently recognised |
Dysstasia 5 |
5
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Eczema 5 |
5
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Erythema multiforme 5 |
5
|
| Nervous system disorders |
E. not currently recognised |
Facial palsy 5 |
5
|
| Nervous system disorders |
E. not currently recognised |
Grand mal convulsion 5 |
5
|
| Reproductive system and breast disorders |
E. not currently recognised |
Menstruation irregular 5 |
5
|
| General disorders and administration site conditions |
E. not currently recognised |
Oedema peripheral 5 |
5
|
| Vascular disorders |
E. not currently recognised |
Pallor 5 |
5
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Sensation of heaviness 5 |
5
|
| Investigations |
E. not currently recognised |
Weight decreased 5 |
5
|
| Psychiatric disorders |
E. not currently recognised |
Anxiety 4 |
4
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Arthralgia 4 |
4
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Blister 4 |
4
|
| Investigations |
E. not currently recognised |
Blood glucose increased 4 |
4
|
| General disorders and administration site conditions |
E. not currently recognised |
Chills 4 |
4
|
| General disorders and administration site conditions |
E. not currently recognised |
Chronic fatigue syndrome 4 |
4
|
| General disorders and administration site conditions |
E. not currently recognised |
Condition aggravated 4 |
4
|
| Psychiatric disorders |
E. not currently recognised |
Confusional state 4 |
4
|
| Injury, poisoning and procedural complications |
E. not currently recognised |
Contusion 4 |
4
|
| Cardiac disorders |
E. not currently recognised |
Cyanosis 4 |
4
|
| Reproductive system and breast disorders |
E. not currently recognised |
Dysmenorrhoea 4 |
4
|
| Nervous system disorders |
E. not currently recognised |
Encephalitis 4 |
4
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Erythema 4 |
4
|
| General disorders and administration site conditions |
E. not currently recognised |
Feeling hot 4 |
4
|
| Nervous system disorders |
E. not currently recognised |
Guillain-barre syndrome 4 |
4
|
| Vascular disorders |
E. not currently recognised |
Hypotension 4 |
4
|
| Nervous system disorders |
E. not currently recognised |
Lethargy 4 |
4
|
| Reproductive system and breast disorders |
E. not currently recognised |
Menorrhagia 4 |
4
|
| Infections and infestations |
E. not currently recognised |
Nasopharyngitis 4 |
4
|
| Gastrointestinal disorders |
E. not currently recognised |
Nausea 4 |
4
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Rash 4 |
4
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Rash 4 |
4
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Skin discolouration 4 |
4
|
| Respiratory, thoracic and mediastinal disorders |
E. not currently recognised |
Wheezing 4 |
4
|
| Surgical and medical procedures |
E. not currently recognised |
Abortion induced 3 |
3
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Alopecia 3 |
3
|
| Nervous system disorders |
E. not currently recognised |
Aphonia 3 |
3
|
| Nervous system disorders |
E. not currently recognised |
Convulsion 3 |
3
|
| Psychiatric disorders |
E. not currently recognised |
Disorientation 3 |
3
|
| Ear and labyrinth disorders |
E. not currently recognised |
Ear pain 3 |
3
|
| Nervous system disorders |
E. not currently recognised |
Epilepsy 3 |
3
|
| General disorders and administration site conditions |
E. not currently recognised |
Feeling abnormal 3 |
3
|
| Nervous system disorders |
E. not currently recognised |
Head discomfort 3 |
3
|
| Nervous system disorders |
E. not currently recognised |
Hemiparesis 3 |
3
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Hyperhidrosis 3 |
3
|
| Infections and infestations |
E. not currently recognised |
Infectious mononucleosis 3 |
3
|
| Pregnancy, puerperium and perinatal conditions |
E. not currently recognised |
Live birth 3 |
3
|
| Reproductive system and breast disorders |
E. not currently recognised |
Menstruation delayed 3 |
3
|
| Gastrointestinal disorders |
E. not currently recognised |
Mouth ulceration 3 |
3
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Muscle twitching 3 |
3
|
| Eye disorders |
E. not currently recognised |
Mydriasis 3 |
3
|
| Vascular disorders |
E. not currently recognised |
Peripheral coldness 3 |
3
|
| Pregnancy, puerperium and perinatal conditions |
E. not currently recognised |
Premature baby 3 |
3
|
| General disorders and administration site conditions |
E. not currently recognised |
Pyrexia 3 |
3
|
| Nervous system disorders |
E. not currently recognised |
Sensory loss 3 |
3
|
| Psychiatric disorders |
E. not currently recognised |
Tearfulness 3 |
3
|
| Nervous system disorders |
E. not currently recognised |
Tremor 3 |
3
|
| Nervous system disorders |
E. not currently recognised |
Unresponsive to stimuli 3 |
3
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Urticaria 3 |
3
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Urticaria chronic 3 |
3
|
| Nervous system disorders |
E. not currently recognised |
Visual field defect 3 |
3
|
| General disorders and administration site conditions |
E. not currently recognised |
Abasia 2 |
2
|
| Gastrointestinal disorders |
E. not currently recognised |
Abdominal pain upper 2 |
2
|
| Psychiatric disorders |
E. not currently recognised |
Abnormal behaviour 2 |
2
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Alopecia areata 2 |
2
|
| Reproductive system and breast disorders |
E. not currently recognised |
Amenorrhoea 2 |
2
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Angioedema 2 |
2
|
| Nervous system disorders |
E. not currently recognised |
Balance disorder 2 |
2
|
| Investigations |
E. not currently recognised |
Body temperature increased 2 |
2
|
| Vascular disorders |
E. not currently recognised |
Circulatory collapse 2 |
2
|
| Nervous system disorders |
E. not currently recognised |
Complex regional pain syndrome 2 |
2
|
| Nervous system disorders |
E. not currently recognised |
Complex regional pain syndrome 2 |
2
|
| Psychiatric disorders |
E. not currently recognised |
Confusional state 2 |
2
|
| Nervous system disorders |
E. not currently recognised |
Crying 2 |
2
|
| Metabolism and nutrition disorders |
E. not currently recognised |
Dehydration 2 |
2
|
| Psychiatric disorders |
E. not currently recognised |
Depressed mood 2 |
2
|
| Nervous system disorders |
E. not currently recognised |
Diplegia 2 |
2
|
| Eye disorders |
E. not currently recognised |
Diplopia 2 |
2
|
| Nervous system disorders |
E. not currently recognised |
Disturbance in attention 2 |
2
|
| Nervous system disorders |
E. not currently recognised |
Dizziness postural 2 |
2
|
| Nervous system disorders |
E. not currently recognised |
Drooling 2 |
2
|
| Injury, poisoning and procedural complications |
E. not currently recognised |
Drug exposure before pregnancy 2 |
2
|
| Nervous system disorders |
E. not currently recognised |
Dysgeusia 2 |
2
|
| Psychiatric disorders |
E. not currently recognised |
Emotional disorder 2 |
2
|
| Eye disorders |
E. not currently recognised |
Eye pain 2 |
2
|
| Nervous system disorders |
E. not currently recognised |
Facial paresis 2 |
2
|
| General disorders and administration site conditions |
E. not currently recognised |
Feeling cold 2 |
2
|
| General disorders and administration site conditions |
E. not currently recognised |
Gait disturbance 2 |
2
|
| General disorders and administration site conditions |
E. not currently recognised |
Gait disturbance 2 |
2
|
| Nervous system disorders |
E. not currently recognised |
Grand mal convulsion 2 |
2
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Groin pain 2 |
2
|
| Respiratory, thoracic and mediastinal disorders |
E. not currently recognised |
Haemoptysis 2 |
2
|
| Vascular disorders |
E. not currently recognised |
Haemorrhage 2 |
2
|
| Infections and infestations |
E. not currently recognised |
Herpes zoster 2 |
2
|
| Infections and infestations |
E. not currently recognised |
Hordeolum 2 |
2
|
| Vascular disorders |
E. not currently recognised |
Hot flush 2 |
2
|
| Respiratory, thoracic and mediastinal disorders |
E. not currently recognised |
Hyperventilation 2 |
2
|
| Nervous system disorders |
E. not currently recognised |
Hypokinesia 2 |
2
|
| Infections and infestations |
E. not currently recognised |
Influenza 2 |
2
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Joint swelling 2 |
2
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Livedo reticularis 2 |
2
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Livedo reticularis 2 |
2
|
| General disorders and administration site conditions |
E. not currently recognised |
Local swelling 2 |
2
|
| Nervous system disorders |
E. not currently recognised |
Loss of consciousness 2 |
2
|
| General disorders and administration site conditions |
E. not currently recognised |
Malaise 2 |
2
|
| Reproductive system and breast disorders |
E. not currently recognised |
Menstrual disorder 2 |
2
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Mobility decreased 2 |
2
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Muscle spasms 2 |
2
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Muscular weakness 2 |
2
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Musculoskeletal pain 2 |
2
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Musculoskeletal stiffness 2 |
2
|
| Nervous system disorders |
E. not currently recognised |
Optic neuritis 2 |
2
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Pain in extremity 2 |
2
|
| Vascular disorders |
E. not currently recognised |
Pallor 2 |
2
|
| Gastrointestinal disorders |
E. not currently recognised |
Paraesthesia oral 2 |
2
|
| Nervous system disorders |
E. not currently recognised |
Petit mal epilepsy 2 |
2
|
| Infections and infestations |
E. not currently recognised |
Pharyngitis 2 |
2
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Photosensitivity reaction 2 |
2
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Photosensitivity reaction 2 |
2
|
| Congenital, familial and genetic disorders |
E. not currently recognised |
Pilonidal cyst congenital 2 |
2
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Purpura 2 |
2
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Rash generalised 2 |
2
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Rheumatoid arthritis 2 |
2
|
| Respiratory, thoracic and mediastinal disorders |
E. not currently recognised |
Rhinorrhoea 2 |
2
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Skin exfoliation 2 |
2
|
| Psychiatric disorders |
E. not currently recognised |
Sleep disorder 2 |
2
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Swelling face 2 |
2
|
| Cardiac disorders |
E. not currently recognised |
Tachycardia 2 |
2
|
| Renal and urinary disorders |
E. not currently recognised |
Urinary incontinence 2 |
2
|
| Renal and urinary disorders |
E. not currently recognised |
Urinary retention 2 |
2
|
| Infections and infestations |
E. not currently recognised |
Urinary tract infection 2 |
2
|
| Ear and labyrinth disorders |
E. not currently recognised |
Vertigo 2 |
2
|
| Eye disorders |
E. not currently recognised |
Visual impairment 2 |
2
|
| Reproductive system and breast disorders |
E. not currently recognised |
Vulval ulceration 2 |
2
|
| Investigations |
E. not currently recognised |
Weight increased 2 |
2
|
| Gastrointestinal disorders |
E. not currently recognised |
Abdominal discomfort 1 |
1
|
| Gastrointestinal disorders |
E. not currently recognised |
Abdominal discomfort 1 |
1
|
| Gastrointestinal disorders |
E. not currently recognised |
Abdominal pain lower 1 |
1
|
| Gastrointestinal disorders |
E. not currently recognised |
Abdominal pain upper 1 |
1
|
| Gastrointestinal disorders |
E. not currently recognised |
Abnormal faeces 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Abnormal sleep-related event 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Abscess 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Acarodermatitis 1 |
1
|
| Eye disorders |
E. not currently recognised |
Accommodation disorder 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Acne 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Acne 1 |
1
|
| Neoplasms benign, malignant and unspecified (incl cysts and polyps) |
E. not currently recognised |
Acute myeloid leukaemia 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Acute psychosis 1 |
1
|
| Respiratory, thoracic and mediastinal disorders |
E. not currently recognised |
Acute respiratory failure 1 |
1
|
| Endocrine disorders |
E. not currently recognised |
Adrenocortical insufficiency acute 1 |
1
|
| Endocrine disorders |
E. not currently recognised |
Adrenocortical insufficiency acute 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Aggression 1 |
1
|
| Investigations |
E. not currently recognised |
Alanine aminotransferase increased 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Alopecia areata 1 |
1
|
| Blood and lymphatic system disorders |
E. not currently recognised |
Anaemia 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Anogenital warts 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Aphasia 1 |
1
|
| Blood and lymphatic system disorders |
E. not currently recognised |
Aplastic anaemia 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Application site pustules 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Areflexia 1 |
1
|
| Congenital, familial and genetic disorders |
E. not currently recognised |
Arteriovenous malformation 1 |
1
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Arthritis 1 |
1
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Arthritis reactive 1 |
1
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Arthropathy 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Asthenia 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Ataxia 1 |
1
|
| Injury, poisoning and procedural complications |
E. not currently recognised |
Axillary nerve injury 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Axillary pain 1 |
1
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Back pain 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Balance disorder 1 |
1
|
| Neoplasms benign, malignant and unspecified (incl cysts and polyps) |
E. not currently recognised |
Benign hydatidiform mole 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Beta haemolytic streptococcal infection 1 |
1
|
| Eye disorders |
E. not currently recognised |
Blindness unilateral 1 |
1
|
| Investigations |
E. not currently recognised |
Blood cortisol decreased 1 |
1
|
| Investigations |
E. not currently recognised |
Blood pressure decreased 1 |
1
|
| Investigations |
E. not currently recognised |
Blood pressure increased 1 |
1
|
| Investigations |
E. not currently recognised |
Body temperature increased 1 |
1
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Bone pain 1 |
1
|
| Reproductive system and breast disorders |
E. not currently recognised |
Breast pain 1 |
1
|
| Reproductive system and breast disorders |
E. not currently recognised |
Breast swelling 1 |
1
|
| Reproductive system and breast disorders |
E. not currently recognised |
Breast tenderness 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Bronchitis 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Burning sensation 1 |
1
|
| Cardiac disorders |
E. not currently recognised |
Cardiac arrest 1 |
1
|
| Investigations |
E. not currently recognised |
Cell marker increased 1 |
1
|
| Congenital, familial and genetic disorders |
E. not currently recognised |
Cerebral palsy 1 |
1
|
| Reproductive system and breast disorders |
E. not currently recognised |
Cervix inflammation 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Chest discomfort 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Chest pain 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Chills 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Chorea 1 |
1
|
| Congenital, familial and genetic disorders |
E. not currently recognised |
Cleft palate 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Cold sweat 1 |
1
|
| Gastrointestinal disorders |
E. not currently recognised |
Colitis 1 |
1
|
| Gastrointestinal disorders |
E. not currently recognised |
Colitis ulcerative 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Condition aggravated 1 |
1
|
| Eye disorders |
E. not currently recognised |
Conjunctival hyperaemia 1 |
1
|
| Gastrointestinal disorders |
E. not currently recognised |
Constipation 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Coordination abnormal 1 |
1
|
| Investigations |
E. not currently recognised |
Csf cell count increased 1 |
1
|
| Eye disorders |
E. not currently recognised |
Dark circles under eyes 1 |
1
|
| Ear and labyrinth disorders |
E. not currently recognised |
Deafness 1 |
1
|
| Ear and labyrinth disorders |
E. not currently recognised |
Deafness bilateral 1 |
1
|
| Metabolism and nutrition disorders |
E. not currently recognised |
Decreased appetite 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Decreased interest 1 |
1
|
| Vascular disorders |
E. not currently recognised |
Deep vein thrombosis 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Depressed level of consciousness 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Depression 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Depression 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Depressive symptom 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Dermatitis allergic 1 |
1
|
| Metabolism and nutrition disorders |
E. not currently recognised |
Diabetes mellitus inadequate control 1 |
1
|
| Metabolism and nutrition disorders |
E. not currently recognised |
Diabetes mellitus inadequate control 1 |
1
|
| Metabolism and nutrition disorders |
E. not currently recognised |
Diabetic ketoacidosis 1 |
1
|
| Gastrointestinal disorders |
E. not currently recognised |
Diarrhoea 1 |
1
|
| Gastrointestinal disorders |
E. not currently recognised |
Diarrhoea haemorrhagic 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Discomfort 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Dissociation 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Dizziness postural 1 |
1
|
| Eye disorders |
E. not currently recognised |
Dry eye 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Dry skin 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Dysgeusia 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Dyskinesia 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Dysphemia 1 |
1
|
| Respiratory, thoracic and mediastinal disorders |
E. not currently recognised |
Dyspnoea 1 |
1
|
| Ear and labyrinth disorders |
E. not currently recognised |
Ear discomfort 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Eating disorder 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Eczema vesicular 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Emotional distress 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Encephalitis 1 |
1
|
| Blood and lymphatic system disorders |
E. not currently recognised |
Eosinophilia 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Erythema 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Erythema multiforme 1 |
1
|
| Eye disorders |
E. not currently recognised |
Excessive eye blinking 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Exercise tolerance decreased 1 |
1
|
| Eye disorders |
E. not currently recognised |
Eye discharge 1 |
1
|
| Eye disorders |
E. not currently recognised |
Eye disorder 1 |
1
|
| Eye disorders |
E. not currently recognised |
Eye pain 1 |
1
|
| Eye disorders |
E. not currently recognised |
Eye swelling 1 |
1
|
| Eye disorders |
E. not currently recognised |
Eyelid oedema 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Facial palsy 1 |
1
|
| Injury, poisoning and procedural complications |
E. not currently recognised |
Fall 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Fear 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Feeling abnormal 1 |
1
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Flank pain 1 |
1
|
| Gastrointestinal disorders |
E. not currently recognised |
Flatulence 1 |
1
|
| Vascular disorders |
E. not currently recognised |
Flushing 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Folliculitis 1 |
1
|
| Gastrointestinal disorders |
E. not currently recognised |
Frequent bowel movements 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Furuncle 1 |
1
|
| Gastrointestinal disorders |
E. not currently recognised |
Gastrointestinal disorder 1 |
1
|
| Eye disorders |
E. not currently recognised |
Gaze palsy 1 |
1
|
| Gastrointestinal disorders |
E. not currently recognised |
Gingival disorder 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Guillain-barre syndrome 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Guttate psoriasis 1 |
1
|
| Blood and lymphatic system disorders |
E. not currently recognised |
Haemolytic uraemic syndrome 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Hallucination, auditory 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Hallucination, visual 1 |
1
|
| Congenital, familial and genetic disorders |
E. not currently recognised |
Heart disease congenital 1 |
1
|
| Investigations |
E. not currently recognised |
Heart rate decreased 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Henoch-schonlein purpura 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Henoch-schonlein purpura 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Hepatitis viral 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Herpes zoster 1 |
1
|
| Ear and labyrinth disorders |
E. not currently recognised |
Hyperacusis 1 |
1
|
| Metabolism and nutrition disorders |
E. not currently recognised |
Hyperglycaemia 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Hyperhidrosis 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Hyperpyrexia 1 |
1
|
| Immune system disorders |
E. not currently recognised |
Hypersensitivity 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Hypertonia 1 |
1
|
| Ear and labyrinth disorders |
E. not currently recognised |
Hypoacusis 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Hypoaesthesia facial 1 |
1
|
| Gastrointestinal disorders |
E. not currently recognised |
Hypoaesthesia oral 1 |
1
|
| Metabolism and nutrition disorders |
E. not currently recognised |
Hypoglycaemia 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Hypomania 1 |
1
|
| Congenital, familial and genetic disorders |
E. not currently recognised |
Hypospadias 1 |
1
|
| Respiratory, thoracic and mediastinal disorders |
E. not currently recognised |
Hypoventilation 1 |
1
|
| Injury, poisoning and procedural complications |
E. not currently recognised |
Inappropriate schedule of drug administration 1 |
1
|
| Injury, poisoning and procedural complications |
E. not currently recognised |
Incorrect dose administered 1 |
1
|
| Metabolism and nutrition disorders |
E. not currently recognised |
Increased appetite 1 |
1
|
| Respiratory, thoracic and mediastinal disorders |
E. not currently recognised |
Increased upper airway secretion 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Infection 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Inflammation 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Injection site erythema 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Injection site injury 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Injection site swelling 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Insomnia 1 |
1
|
| Gastrointestinal disorders |
E. not currently recognised |
Intestinal functional disorder 1 |
1
|
| Gastrointestinal disorders |
E. not currently recognised |
Irritable bowel syndrome 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Ivth nerve paralysis 1 |
1
|
| Hepatobiliary disorders |
E. not currently recognised |
Jaundice 1 |
1
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Joint stiffness 1 |
1
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Joint stiffness 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Kidney infection 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Labyrinthitis 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Laryngitis 1 |
1
|
| Congenital, familial and genetic disorders |
E. not currently recognised |
Limb malformation 1 |
1
|
| Gastrointestinal disorders |
E. not currently recognised |
Lip blister 1 |
1
|
| Gastrointestinal disorders |
E. not currently recognised |
Lip swelling 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Local swelling 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Meningism 1 |
1
|
| Reproductive system and breast disorders |
E. not currently recognised |
Menorrhagia 1 |
1
|
| Reproductive system and breast disorders |
E. not currently recognised |
Menstrual disorder 1 |
1
|
| Reproductive system and breast disorders |
E. not currently recognised |
Menstruation delayed 1 |
1
|
| Reproductive system and breast disorders |
E. not currently recognised |
Menstruation irregular 1 |
1
|
| Reproductive system and breast disorders |
E. not currently recognised |
Metrorrhagia 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Migraine 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Migraine with aura 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Molluscum contagiosum 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Monoplegia 1 |
1
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Muscle rigidity 1 |
1
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Muscle twitching 1 |
1
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Musculoskeletal chest pain 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Myoclonic epilepsy 1 |
1
|
| Respiratory, thoracic and mediastinal disorders |
E. not currently recognised |
Nasal congestion 1 |
1
|
| Neoplasms benign, malignant and unspecified (incl cysts and polyps) |
E. not currently recognised |
Neoplasm malignant 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Neuritis 1 |
1
|
| Renal and urinary disorders |
E. not currently recognised |
Neurogenic bladder 1 |
1
|
| Blood and lymphatic system disorders |
E. not currently recognised |
Neutropenia 1 |
1
|
| Investigations |
E. not currently recognised |
Neutrophil count decreased 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Oedema peripheral 1 |
1
|
| Respiratory, thoracic and mediastinal disorders |
E. not currently recognised |
Oropharyngeal blistering 1 |
1
|
| Respiratory, thoracic and mediastinal disorders |
E. not currently recognised |
Oropharyngeal pain 1 |
1
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Osteitis 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Otitis media 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Pain 1 |
1
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Palindromic rheumatism 1 |
1
|
| Blood and lymphatic system disorders |
E. not currently recognised |
Pancytopenia 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Paralysis 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Paranoia 1 |
1
|
| Investigations |
E. not currently recognised |
Peak expiratory flow rate decreased 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Petechiae 1 |
1
|
| Eye disorders |
E. not currently recognised |
Photopsia 1 |
1
|
| Investigations |
E. not currently recognised |
Platelet count decreased 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Pneumonia viral 1 |
1
|
| Renal and urinary disorders |
E. not currently recognised |
Pollakiuria 1 |
1
|
| Pregnancy, puerperium and perinatal conditions |
E. not currently recognised |
Pregnancy with injectable contraceptive 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Presyncope 1 |
1
|
| Respiratory, thoracic and mediastinal disorders |
E. not currently recognised |
Productive cough 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Psoriasis 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Psychiatric symptom 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Psychomotor hyperactivity 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Psychotic disorder 1 |
1
|
| Investigations |
E. not currently recognised |
Radial pulse 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Radiculitis brachial 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Rash erythematous 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Rash maculo-papular 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Rash vesicular 1 |
1
|
| Renal and urinary disorders |
E. not currently recognised |
Renal failure 1 |
1
|
| Investigations |
E. not currently recognised |
Respiratory rate increased 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Respiratory syncytial virus infection 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Respiratory tract infection 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Screaming 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Sedation 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Sensation of foreign body 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Sensation of pressure 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Sensory loss 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Sepsis 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Severe acute respiratory syndrome 1 |
1
|
| Cardiac disorders |
E. not currently recognised |
Sinus tachycardia 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Skin burning sensation 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Skin disorder 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Skin hypertrophy 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Skin infection 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Skin irritation 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Skin lesion 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Somatisation disorder 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Somnolence 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Speech disorder 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Staphylococcal infection 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Status epilepticus 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Streptococcal sepsis 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Swelling 1 |
1
|
| Gastrointestinal disorders |
E. not currently recognised |
Swollen tongue 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Systemic inflammatory response syndrome 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Temperature intolerance 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Tenderness 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Thirst 1 |
1
|
| Respiratory, thoracic and mediastinal disorders |
E. not currently recognised |
Throat tightness 1 |
1
|
| Ear and labyrinth disorders |
E. not currently recognised |
Tinnitus 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Trichorrhexis 1 |
1
|
| Metabolism and nutrition disorders |
E. not currently recognised |
Type 1 diabetes mellitus 1 |
1
|
| Respiratory, thoracic and mediastinal disorders |
E. not currently recognised |
Upper airway obstruction 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Upper respiratory tract infection 1 |
1
|
| Renal and urinary disorders |
E. not currently recognised |
Urinary retention 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Urticaria 1 |
1
|
| Reproductive system and breast disorders |
E. not currently recognised |
Vaginal discharge 1 |
1
|
| Reproductive system and breast disorders |
E. not currently recognised |
Vaginal lesion 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Varicella 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Viraemia 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Vitiligo 1 |
1
|
| Eye disorders |
E. not currently recognised |
Vitreous floaters 1 |
1
|
| Gastrointestinal disorders |
E. not currently recognised |
Vomiting 1 |
1
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Weight bearing difficulty 1 |
1
|
| Investigations |
E. not currently recognised |
Weight decreased 1 |
1
|
| Respiratory, thoracic and mediastinal disorders |
E. not currently recognised |
Wheezing 1 |
1
|
| Injury, poisoning and procedural complications |
E. not currently recognised |
Wrong technique in drug usage process 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Yellow skin 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Stevens-johnson syndrome 1 |
|













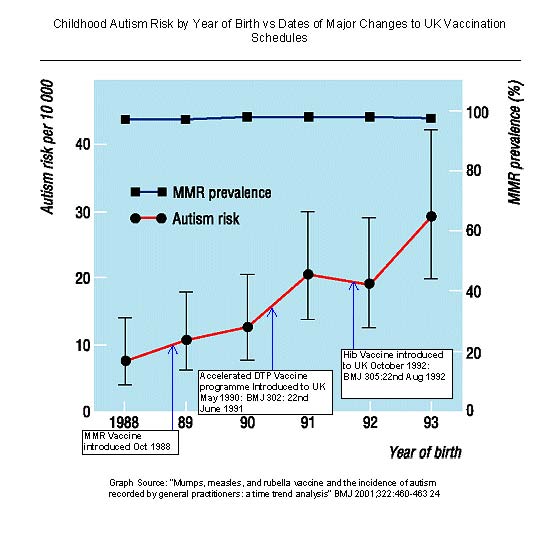















 Some are calling this “‘compromise’, because most things in Montpelier are about ‘compromise’.” I disagree.
Some are calling this “‘compromise’, because most things in Montpelier are about ‘compromise’.” I disagree.






































In our post above noting direct censorship of public facts by The Guardian perhaps we should have added “Follow the Money”.
GUARDIAN & BRITISH MEDICAL JOURNAL
Guardian partners with British Medical Journal Group for online first Tuesday 3 March 2009 00.00 GMT
BRITISH MEDICAL JOURNAL & DRUG INDUSTRY
The Editor in Chief of the British Medical Journal was forced to make an embarrassing correction regarding the BMJ’s own failures to disclose its conflicting financial interests in the drug industry.
Here is the correction forced ultimately by online criticism from New York charity The Alliance for Human Research Protection:-
However, this also still fails to mention the most glaring conflict of all, which it all – BMJ’s business partnership with Merck through their information arm, Univadis (‘MSD signs partnership with BMJ group’).