| System Organ Class |
Category A to E |
Reported event (Preferred Term) |
Number of cases
|
|
A. Injection-site reactions |
Pain in extremity 485 |
485
|
|
A. Injection-site reactions |
Injection site swelling 113 |
113
|
|
A. Injection-site reactions |
Oedema peripheral 109 |
109
|
|
A. Injection-site reactions |
Limb discomfort 106 |
106
|
|
A. Injection-site reactions |
Hypoaesthesia 105 |
105
|
|
A. Injection-site reactions |
Injection site erythema 85 |
85
|
|
A. Injection-site reactions |
Injection site pain 81 |
81
|
|
A. Injection-site reactions |
Erythema 45 |
45
|
|
A. Injection-site reactions |
Paraesthesia 37 |
37
|
|
A. Injection-site reactions |
Skin discolouration 33 |
33
|
|
A. Injection-site reactions |
Injection site rash 32 |
32
|
|
A. Injection-site reactions |
Injection site mass 29 |
29
|
|
A. Injection-site reactions |
Injection site reaction 26 |
26
|
|
A. Injection-site reactions |
Pain 23 |
23
|
|
A. Injection-site reactions |
Contusion 21 |
21
|
|
A. Injection-site reactions |
Musculoskeletal stiffness 21 |
21
|
|
A. Injection-site reactions |
Peripheral coldness 20 |
20
|
|
A. Injection-site reactions |
Local reaction 19 |
19
|
|
A. Injection-site reactions |
Injection site inflammation 18 |
18
|
|
A. Injection-site reactions |
Injection site warmth 18 |
18
|
|
A. Injection-site reactions |
Pain in extremity 16 |
16
|
|
A. Injection-site reactions |
Local swelling 15 |
15
|
|
A. Injection-site reactions |
Sensation of heaviness 15 |
15
|
|
A. Injection-site reactions |
Injection site haematoma 12 |
12
|
|
A. Injection-site reactions |
Injection site pruritus 11 |
11
|
|
A. Injection-site reactions |
Rash macular 10 |
10
|
|
A. Injection-site reactions |
Oedema peripheral 9 |
9
|
|
A. Injection-site reactions |
Feeling cold 8 |
8
|
|
A. Injection-site reactions |
Injection site induration 8 |
8
|
|
A. Injection-site reactions |
Injection site nodule 8 |
8
|
|
A. Injection-site reactions |
Livedo reticularis 8 |
8
|
|
A. Injection-site reactions |
Swelling 8 |
8
|
|
A. Injection-site reactions |
Injection site anaesthesia 6 |
6
|
|
A. Injection-site reactions |
Injection site swelling 6 |
6
|
|
A. Injection-site reactions |
Muscular weakness 6 |
6
|
|
A. Injection-site reactions |
Myalgia 6 |
6
|
|
A. Injection-site reactions |
Neck pain 6 |
6
|
|
A. Injection-site reactions |
Pain 6 |
6
|
|
A. Injection-site reactions |
Rash 6 |
6
|
|
A. Injection-site reactions |
Erythema 5 |
5
|
|
A. Injection-site reactions |
Feeling hot 5 |
5
|
|
A. Injection-site reactions |
Injection site erythema 5 |
5
|
|
A. Injection-site reactions |
Pruritus 5 |
5
|
|
A. Injection-site reactions |
Cyanosis 4 |
4
|
|
A. Injection-site reactions |
Feeling abnormal 4 |
4
|
|
A. Injection-site reactions |
Injection site infection 4 |
4
|
|
A. Injection-site reactions |
Musculoskeletal stiffness 4 |
4
|
|
A. Injection-site reactions |
Pallor 4 |
4
|
|
A. Injection-site reactions |
Sensory disturbance 4 |
4
|
|
A. Injection-site reactions |
Tenderness 4 |
4
|
|
A. Injection-site reactions |
Asthenia 3 |
3
|
|
A. Injection-site reactions |
Feeling hot 3 |
3
|
|
A. Injection-site reactions |
Inflammation 3 |
3
|
|
A. Injection-site reactions |
Injection site discharge 3 |
3
|
|
A. Injection-site reactions |
Injection site discolouration 3 |
3
|
|
A. Injection-site reactions |
Injection site irritation 3 |
3
|
|
A. Injection-site reactions |
Injection site reaction 3 |
3
|
|
A. Injection-site reactions |
Injection site urticaria 3 |
3
|
|
A. Injection-site reactions |
Injection site vesicles 3 |
3
|
|
A. Injection-site reactions |
Limb immobilisation 3 |
3
|
|
A. Injection-site reactions |
Musculoskeletal pain 3 |
3
|
|
A. Injection-site reactions |
Poor peripheral circulation 3 |
3
|
|
A. Injection-site reactions |
Sensory loss 3 |
3
|
|
A. Injection-site reactions |
Skin warm 3 |
3
|
|
A. Injection-site reactions |
Dry skin 2 |
2
|
|
A. Injection-site reactions |
Grip strength decreased 2 |
2
|
|
A. Injection-site reactions |
Hypoaesthesia 2 |
2
|
|
A. Injection-site reactions |
Injected limb mobility decreased 2 |
2
|
|
A. Injection-site reactions |
Injection site cellulitis 2 |
2
|
|
A. Injection-site reactions |
Injection site coldness 2 |
2
|
|
A. Injection-site reactions |
Injection site discolouration 2 |
2
|
|
A. Injection-site reactions |
Injection site mass 2 |
2
|
|
A. Injection-site reactions |
Injection site pain 2 |
2
|
|
A. Injection-site reactions |
Peripheral coldness 2 |
2
|
|
A. Injection-site reactions |
Pruritus 2 |
2
|
|
A. Injection-site reactions |
Sensory loss 2 |
2
|
|
A. Injection-site reactions |
Skin discolouration 2 |
2
|
|
A. Injection-site reactions |
Skin reaction 2 |
2
|
|
A. Injection-site reactions |
Skin reaction 2 |
2
|
|
A. Injection-site reactions |
Tenderness 2 |
2
|
|
A. Injection-site reactions |
Blister 1 |
1
|
|
A. Injection-site reactions |
Complex regional pain syndrome 1 |
1
|
|
A. Injection-site reactions |
Extensive swelling of vaccinated limb 1 |
1
|
|
A. Injection-site reactions |
Hyperaesthesia 1 |
1
|
|
A. Injection-site reactions |
Hyperaesthesia 1 |
1
|
|
A. Injection-site reactions |
Hypokinesia 1 |
1
|
|
A. Injection-site reactions |
Hypokinesia 1 |
1
|
|
A. Injection-site reactions |
Immobile 1 |
1
|
|
A. Injection-site reactions |
Impetigo 1 |
1
|
|
A. Injection-site reactions |
Injection site abscess 1 |
1
|
|
A. Injection-site reactions |
Injection site anaesthesia 1 |
1
|
|
A. Injection-site reactions |
Injection site coldness 1 |
1
|
|
A. Injection-site reactions |
Injection site discomfort 1 |
1
|
|
A. Injection-site reactions |
Injection site haematoma 1 |
1
|
|
A. Injection-site reactions |
Injection site haemorrhage 1 |
1
|
|
A. Injection-site reactions |
Injection site haemorrhage 1 |
1
|
|
A. Injection-site reactions |
Injection site joint movement impairment 1 |
1
|
|
A. Injection-site reactions |
Injection site joint pain 1 |
1
|
|
A. Injection-site reactions |
Injection site movement impairment 1 |
1
|
|
A. Injection-site reactions |
Injection site movement impairment 1 |
1
|
|
A. Injection-site reactions |
Injection site papule 1 |
1
|
|
A. Injection-site reactions |
Injection site paraesthesia 1 |
1
|
|
A. Injection-site reactions |
Injection site rash 1 |
1
|
|
A. Injection-site reactions |
Injection site scab 1 |
1
|
|
A. Injection-site reactions |
Joint swelling 1 |
1
|
|
A. Injection-site reactions |
Limb immobilisation 1 |
1
|
|
A. Injection-site reactions |
Local reaction 1 |
1
|
|
A. Injection-site reactions |
Local swelling 1 |
1
|
|
A. Injection-site reactions |
Lymphoedema 1 |
1
|
|
A. Injection-site reactions |
Mass 1 |
1
|
|
A. Injection-site reactions |
Mobility decreased 1 |
1
|
|
A. Injection-site reactions |
Muscle rigidity 1 |
1
|
|
A. Injection-site reactions |
Muscle spasms 1 |
1
|
|
A. Injection-site reactions |
Muscle tightness 1 |
1
|
|
A. Injection-site reactions |
Musculoskeletal pain 1 |
1
|
|
A. Injection-site reactions |
Nausea 1 |
1
|
|
A. Injection-site reactions |
Nodule 1 |
1
|
|
A. Injection-site reactions |
Pain of skin 1 |
1
|
|
A. Injection-site reactions |
Paraesthesia 1 |
1
|
|
A. Injection-site reactions |
Peripheral vascular disorder 1 |
1
|
|
A. Injection-site reactions |
Rash 1 |
1
|
|
A. Injection-site reactions |
Rash maculo-papular 1 |
1
|
|
A. Injection-site reactions |
Rash pruritic 1 |
1
|
|
A. Injection-site reactions |
Scab 1 |
1
|
|
A. Injection-site reactions |
Sensation of heaviness 1 |
1
|
|
A. Injection-site reactions |
Sensation of pressure 1 |
1
|
|
A. Injection-site reactions |
Tremor 1 |
1
|
|
A. Injection-site reactions |
Urticaria 1 |
1
|
|
A. Injection-site reactions |
Urticaria 1 |
1
|
|
B. Allergic reactions |
Rash 130 |
130
|
|
B. Allergic reactions |
Urticaria 89 |
89
|
|
B. Allergic reactions |
Pruritus 60 |
60
|
|
B. Allergic reactions |
Erythema 47 |
47
|
|
B. Allergic reactions |
Swelling face 42 |
42
|
|
B. Allergic reactions |
Anaphylactic reaction 41 |
41
|
|
B. Allergic reactions |
Dyspnoea 33 |
33
|
|
B. Allergic reactions |
Rash generalised 31 |
31
|
|
B. Allergic reactions |
Rash pruritic 31 |
31
|
|
B. Allergic reactions |
Oedema peripheral 29 |
29
|
|
B. Allergic reactions |
Lip swelling 26 |
26
|
|
B. Allergic reactions |
Rash macular 24 |
24
|
|
B. Allergic reactions |
Dizziness 23 |
23
|
|
B. Allergic reactions |
Hypersensitivity 22 |
22
|
|
B. Allergic reactions |
Eye swelling 18 |
18
|
|
B. Allergic reactions |
Paraesthesia oral 17 |
17
|
|
B. Allergic reactions |
Malaise 15 |
15
|
|
B. Allergic reactions |
Throat tightness 14 |
14
|
|
B. Allergic reactions |
Rash 13 |
13
|
|
B. Allergic reactions |
Swollen tongue 13 |
13
|
|
B. Allergic reactions |
Chest discomfort 11 |
11
|
|
B. Allergic reactions |
Rash erythematous 11 |
11
|
|
B. Allergic reactions |
Feeling hot 9 |
9
|
|
B. Allergic reactions |
Flushing 9 |
9
|
|
B. Allergic reactions |
Pruritus generalised 9 |
9
|
|
B. Allergic reactions |
Dermatitis allergic 8 |
8
|
|
B. Allergic reactions |
Pallor 8 |
8
|
|
B. Allergic reactions |
Pharyngeal oedema 8 |
8
|
|
B. Allergic reactions |
Urticaria 8 |
8
|
|
B. Allergic reactions |
Fatigue 7 |
7
|
|
B. Allergic reactions |
Oropharyngeal pain 7 |
7
|
|
B. Allergic reactions |
Paraesthesia 7 |
7
|
|
B. Allergic reactions |
Angioedema 6 |
6
|
|
B. Allergic reactions |
Dysphagia 6 |
6
|
|
B. Allergic reactions |
Headache 6 |
6
|
|
B. Allergic reactions |
Inflammation 6 |
6
|
|
B. Allergic reactions |
Pyrexia 6 |
6
|
|
B. Allergic reactions |
Throat irritation 6 |
6
|
|
B. Allergic reactions |
Blister 5 |
5
|
|
B. Allergic reactions |
Dyspnoea 5 |
5
|
|
B. Allergic reactions |
Hyperventilation 5 |
5
|
|
B. Allergic reactions |
Hypoaesthesia oral 5 |
5
|
|
B. Allergic reactions |
Vomiting 5 |
5
|
|
B. Allergic reactions |
Wheezing 5 |
5
|
|
B. Allergic reactions |
Anaphylactic shock 4 |
4
|
|
B. Allergic reactions |
Eyelid oedema 4 |
4
|
|
B. Allergic reactions |
Hypersensitivity 4 |
4
|
|
B. Allergic reactions |
Hypoaesthesia 4 |
4
|
|
B. Allergic reactions |
Local swelling 4 |
4
|
|
B. Allergic reactions |
Nausea 4 |
4
|
|
B. Allergic reactions |
Pain in extremity 4 |
4
|
|
B. Allergic reactions |
Dermatitis allergic 3 |
3
|
|
B. Allergic reactions |
Erythema 3 |
3
|
|
B. Allergic reactions |
Eye pruritus 3 |
3
|
|
B. Allergic reactions |
Eyelid oedema 3 |
3
|
|
B. Allergic reactions |
Hyperhidrosis 3 |
3
|
|
B. Allergic reactions |
Laryngeal oedema 3 |
3
|
|
B. Allergic reactions |
Limb discomfort 3 |
3
|
|
B. Allergic reactions |
Nasopharyngitis 3 |
3
|
|
B. Allergic reactions |
Ocular hyperaemia 3 |
3
|
|
B. Allergic reactions |
Pain 3 |
3
|
|
B. Allergic reactions |
Petechiae 3 |
3
|
|
B. Allergic reactions |
Rash erythematous 3 |
3
|
|
B. Allergic reactions |
Rash macular 3 |
3
|
|
B. Allergic reactions |
Rash maculo-papular 3 |
3
|
|
B. Allergic reactions |
Rash pruritic 3 |
3
|
|
B. Allergic reactions |
Skin irritation 3 |
3
|
|
B. Allergic reactions |
Skin reaction 3 |
3
|
|
B. Allergic reactions |
Somnolence 3 |
3
|
|
B. Allergic reactions |
Swelling 3 |
3
|
|
B. Allergic reactions |
Vision blurred 3 |
3
|
|
B. Allergic reactions |
Abdominal pain 2 |
2
|
|
B. Allergic reactions |
Abdominal pain upper 2 |
2
|
|
B. Allergic reactions |
Anaphylactic reaction 2 |
2
|
|
B. Allergic reactions |
Blister 2 |
2
|
|
B. Allergic reactions |
Body temperature increased 2 |
2
|
|
B. Allergic reactions |
Cold sweat 2 |
2
|
|
B. Allergic reactions |
Dermatitis contact 2 |
2
|
|
B. Allergic reactions |
Dizziness 2 |
2
|
|
B. Allergic reactions |
Face oedema 2 |
2
|
|
B. Allergic reactions |
Feeling cold 2 |
2
|
|
B. Allergic reactions |
Heart rate increased 2 |
2
|
|
B. Allergic reactions |
Heart rate irregular 2 |
2
|
|
B. Allergic reactions |
Heat rash 2 |
2
|
|
B. Allergic reactions |
Lip swelling 2 |
2
|
|
B. Allergic reactions |
Peripheral coldness 2 |
2
|
|
B. Allergic reactions |
Pharyngeal oedema 2 |
2
|
|
B. Allergic reactions |
Pruritus 2 |
2
|
|
B. Allergic reactions |
Rash generalised 2 |
2
|
|
B. Allergic reactions |
Skin discolouration 2 |
2
|
|
B. Allergic reactions |
Skin disorder 2 |
2
|
|
B. Allergic reactions |
Swollen tongue 2 |
2
|
|
B. Allergic reactions |
Tachycardia 2 |
2
|
|
B. Allergic reactions |
Type i hypersensitivity 2 |
2
|
|
B. Allergic reactions |
Anaphylactoid reaction 1 |
1
|
|
B. Allergic reactions |
Asthenia 1 |
1
|
|
B. Allergic reactions |
Asthenopia 1 |
1
|
|
B. Allergic reactions |
Asthma 1 |
1
|
|
B. Allergic reactions |
Back pain 1 |
1
|
|
B. Allergic reactions |
Breath sounds abnormal 1 |
1
|
|
B. Allergic reactions |
Bronchospasm 1 |
1
|
|
B. Allergic reactions |
Chest pain 1 |
1
|
|
B. Allergic reactions |
Chills 1 |
1
|
|
B. Allergic reactions |
Condition aggravated 1 |
1
|
|
B. Allergic reactions |
Confusional state 1 |
1
|
|
B. Allergic reactions |
Conjunctival hyperaemia 1 |
1
|
|
B. Allergic reactions |
Contusion 1 |
1
|
|
B. Allergic reactions |
Convulsion 1 |
1
|
|
B. Allergic reactions |
Cough 1 |
1
|
|
B. Allergic reactions |
Dermatitis 1 |
1
|
|
B. Allergic reactions |
Dry throat 1 |
1
|
|
B. Allergic reactions |
Dysphagia 1 |
1
|
|
B. Allergic reactions |
Eczema 1 |
1
|
|
B. Allergic reactions |
Eczema 1 |
1
|
|
B. Allergic reactions |
Eyelid disorder 1 |
1
|
|
B. Allergic reactions |
Eyes sunken 1 |
1
|
|
B. Allergic reactions |
Fatigue 1 |
1
|
|
B. Allergic reactions |
Feeling abnormal 1 |
1
|
|
B. Allergic reactions |
Feeling hot 1 |
1
|
|
B. Allergic reactions |
Feeling jittery 1 |
1
|
|
B. Allergic reactions |
Generalised erythema 1 |
1
|
|
B. Allergic reactions |
Gingival swelling 1 |
1
|
|
B. Allergic reactions |
Headache 1 |
1
|
|
B. Allergic reactions |
Hypersomnia 1 |
1
|
|
B. Allergic reactions |
Hypertension 1 |
1
|
|
B. Allergic reactions |
Hypoventilation 1 |
1
|
|
B. Allergic reactions |
Increased bronchial secretion 1 |
1
|
|
B. Allergic reactions |
Infusion site swelling 1 |
1
|
|
B. Allergic reactions |
Laryngeal oedema 1 |
1
|
|
B. Allergic reactions |
Lethargy 1 |
1
|
|
B. Allergic reactions |
Lip blister 1 |
1
|
|
B. Allergic reactions |
Lip ulceration 1 |
1
|
|
B. Allergic reactions |
Local reaction 1 |
1
|
|
B. Allergic reactions |
Loss of consciousness 1 |
1
|
|
B. Allergic reactions |
Migraine 1 |
1
|
|
B. Allergic reactions |
Muscle tightness 1 |
1
|
|
B. Allergic reactions |
Musculoskeletal stiffness 1 |
1
|
|
B. Allergic reactions |
Myalgia 1 |
1
|
|
B. Allergic reactions |
Mydriasis 1 |
1
|
|
B. Allergic reactions |
Nausea 1 |
1
|
|
B. Allergic reactions |
Neck pain 1 |
1
|
|
B. Allergic reactions |
Oedema mouth 1 |
1
|
|
B. Allergic reactions |
Oedema mouth 1 |
1
|
|
B. Allergic reactions |
Oesophageal discomfort 1 |
1
|
|
B. Allergic reactions |
Oral discomfort 1 |
1
|
|
B. Allergic reactions |
Oral pain 1 |
1
|
|
B. Allergic reactions |
Palpitations 1 |
1
|
|
B. Allergic reactions |
Panic reaction 1 |
1
|
|
B. Allergic reactions |
Paraesthesia oral 1 |
1
|
|
B. Allergic reactions |
Periorbital oedema 1 |
1
|
|
B. Allergic reactions |
Photophobia 1 |
1
|
|
B. Allergic reactions |
Piloerection 1 |
1
|
|
B. Allergic reactions |
Pulse absent 1 |
1
|
|
B. Allergic reactions |
Purpura 1 |
1
|
|
B. Allergic reactions |
Pyrexia 1 |
1
|
|
B. Allergic reactions |
Rash follicular 1 |
1
|
|
B. Allergic reactions |
Rash papular 1 |
1
|
|
B. Allergic reactions |
Respiratory rate increased 1 |
1
|
|
B. Allergic reactions |
Sensation of foreign body 1 |
1
|
|
B. Allergic reactions |
Sneezing 1 |
1
|
|
B. Allergic reactions |
Somnolence 1 |
1
|
|
B. Allergic reactions |
Speech disorder 1 |
1
|
|
B. Allergic reactions |
Stridor 1 |
1
|
|
B. Allergic reactions |
Swelling 1 |
1
|
|
B. Allergic reactions |
Swelling face 1 |
1
|
|
B. Allergic reactions |
Syncope 1 |
1
|
|
B. Allergic reactions |
Systemic lupus erythematosus rash 1 |
1
|
|
B. Allergic reactions |
Tenderness 1 |
1
|
|
B. Allergic reactions |
Thirst 1 |
1
|
|
B. Allergic reactions |
Throat irritation 1 |
1
|
|
B. Allergic reactions |
Throat tightness 1 |
1
|
|
B. Allergic reactions |
Tremor 1 |
1
|
|
B. Allergic reactions |
Type IV hypersensitivity reaction 1 |
1
|
|
B. Allergic reactions |
Urticaria pigmentosa 1 |
1
|
|
B. Allergic reactions |
Visual impairment 1 |
1
|
|
B. Allergic reactions |
Vomiting 1 |
1
|
|
C. ‘Psychogenic’ events |
Dizziness 327 |
327
|
|
C. ‘Psychogenic’ events |
Syncope 296 |
296
|
|
C. ‘Psychogenic’ events |
Nausea 151 |
151
|
|
C. ‘Psychogenic’ events |
Headache 109 |
109
|
|
C. ‘Psychogenic’ events |
Pallor 108 |
108
|
|
C. ‘Psychogenic’ events |
Vomiting 77 |
77
|
|
C. ‘Psychogenic’ events |
Malaise 74 |
74
|
|
C. ‘Psychogenic’ events |
Tremor 61 |
61
|
|
C. ‘Psychogenic’ events |
Vision blurred 46 |
46
|
|
C. ‘Psychogenic’ events |
Feeling hot 45 |
45
|
|
C. ‘Psychogenic’ events |
Flushing 40 |
40
|
|
C. ‘Psychogenic’ events |
Cold sweat 35 |
35
|
|
C. ‘Psychogenic’ events |
Syncope 27 |
27
|
|
C. ‘Psychogenic’ events |
Hyperhidrosis 25 |
25
|
|
C. ‘Psychogenic’ events |
Presyncope 23 |
23
|
|
C. ‘Psychogenic’ events |
Hyperventilation 21 |
21
|
|
C. ‘Psychogenic’ events |
Loss of consciousness 19 |
19
|
|
C. ‘Psychogenic’ events |
Dyspnoea 18 |
18
|
|
C. ‘Psychogenic’ events |
Paraesthesia 18 |
18
|
|
C. ‘Psychogenic’ events |
Chills 17 |
17
|
|
C. ‘Psychogenic’ events |
Convulsion 17 |
17
|
|
C. ‘Psychogenic’ events |
Pyrexia 16 |
16
|
|
C. ‘Psychogenic’ events |
Somnolence 16 |
16
|
|
C. ‘Psychogenic’ events |
Dizziness 15 |
15
|
|
C. ‘Psychogenic’ events |
Fatigue 15 |
15
|
|
C. ‘Psychogenic’ events |
Heart rate increased 14 |
14
|
|
C. ‘Psychogenic’ events |
Unresponsive to stimuli 14 |
14
|
|
C. ‘Psychogenic’ events |
Muscle twitching 13 |
13
|
|
C. ‘Psychogenic’ events |
Rash 13 |
13
|
|
C. ‘Psychogenic’ events |
Asthenia 12 |
12
|
|
C. ‘Psychogenic’ events |
Feeling cold 12 |
12
|
|
C. ‘Psychogenic’ events |
Hypoaesthesia 12 |
12
|
|
C. ‘Psychogenic’ events |
Panic attack 12 |
12
|
|
C. ‘Psychogenic’ events |
Chest discomfort 11 |
11
|
|
C. ‘Psychogenic’ events |
Dyskinesia 11 |
11
|
|
C. ‘Psychogenic’ events |
Eye rolling 11 |
11
|
|
C. ‘Psychogenic’ events |
Tachycardia 11 |
11
|
|
C. ‘Psychogenic’ events |
Tearfulness 11 |
11
|
|
C. ‘Psychogenic’ events |
Nervousness 10 |
10
|
|
C. ‘Psychogenic’ events |
Erythema 9 |
9
|
|
C. ‘Psychogenic’ events |
Headache 9 |
9
|
|
C. ‘Psychogenic’ events |
Rash macular 9 |
9
|
|
C. ‘Psychogenic’ events |
Abdominal pain 8 |
8
|
|
C. ‘Psychogenic’ events |
Chest pain 8 |
8
|
|
C. ‘Psychogenic’ events |
Peripheral coldness 8 |
8
|
|
C. ‘Psychogenic’ events |
Abdominal pain upper 7 |
7
|
|
C. ‘Psychogenic’ events |
Anxiety 7 |
7
|
|
C. ‘Psychogenic’ events |
Fall 7 |
7
|
|
C. ‘Psychogenic’ events |
Hypotension 7 |
7
|
|
C. ‘Psychogenic’ events |
Lethargy 7 |
7
|
|
C. ‘Psychogenic’ events |
Muscular weakness 7 |
7
|
|
C. ‘Psychogenic’ events |
Photophobia 7 |
7
|
|
C. ‘Psychogenic’ events |
Visual impairment 7 |
7
|
|
C. ‘Psychogenic’ events |
Confusional state 6 |
6
|
|
C. ‘Psychogenic’ events |
Deafness 6 |
6
|
|
C. ‘Psychogenic’ events |
Feeling of body temperature change 6 |
6
|
|
C. ‘Psychogenic’ events |
Muscle rigidity 6 |
6
|
|
C. ‘Psychogenic’ events |
Musculoskeletal stiffness 6 |
6
|
|
C. ‘Psychogenic’ events |
Mydriasis 6 |
6
|
|
C. ‘Psychogenic’ events |
Nasopharyngitis 6 |
6
|
|
C. ‘Psychogenic’ events |
Throat tightness 6 |
6
|
|
C. ‘Psychogenic’ events |
Dizziness postural 5 |
5
|
|
C. ‘Psychogenic’ events |
Dysgeusia 5 |
5
|
|
C. ‘Psychogenic’ events |
Feeling abnormal 5 |
5
|
|
C. ‘Psychogenic’ events |
Pallor 5 |
5
|
|
C. ‘Psychogenic’ events |
Skin discolouration 5 |
5
|
|
C. ‘Psychogenic’ events |
Urticaria 5 |
5
|
|
C. ‘Psychogenic’ events |
Abdominal discomfort 4 |
4
|
|
C. ‘Psychogenic’ events |
Blindness transient 4 |
4
|
|
C. ‘Psychogenic’ events |
Body temperature increased 4 |
4
|
|
C. ‘Psychogenic’ events |
Decreased appetite 4 |
4
|
|
C. ‘Psychogenic’ events |
Hot flush 4 |
4
|
|
C. ‘Psychogenic’ events |
Migraine 4 |
4
|
|
C. ‘Psychogenic’ events |
Muscle spasms 4 |
4
|
|
C. ‘Psychogenic’ events |
Pulse abnormal 4 |
4
|
|
C. ‘Psychogenic’ events |
Respiratory rate increased 4 |
4
|
|
C. ‘Psychogenic’ events |
Tinnitus 4 |
4
|
|
C. ‘Psychogenic’ events |
Urinary incontinence 4 |
4
|
|
C. ‘Psychogenic’ events |
Vomiting 4 |
4
|
|
C. ‘Psychogenic’ events |
Abasia 3 |
3
|
|
C. ‘Psychogenic’ events |
Agitation 3 |
3
|
|
C. ‘Psychogenic’ events |
Balance disorder 3 |
3
|
|
C. ‘Psychogenic’ events |
Blindness 3 |
3
|
|
C. ‘Psychogenic’ events |
Blood pressure decreased 3 |
3
|
|
C. ‘Psychogenic’ events |
Cyanosis 3 |
3
|
|
C. ‘Psychogenic’ events |
Disorientation 3 |
3
|
|
C. ‘Psychogenic’ events |
Disturbance in attention 3 |
3
|
|
C. ‘Psychogenic’ events |
Dyspnoea 3 |
3
|
|
C. ‘Psychogenic’ events |
Dysstasia 3 |
3
|
|
C. ‘Psychogenic’ events |
Emotional disorder 3 |
3
|
|
C. ‘Psychogenic’ events |
Feeling drunk 3 |
3
|
|
C. ‘Psychogenic’ events |
Hearing impaired 3 |
3
|
|
C. ‘Psychogenic’ events |
Heart rate irregular 3 |
3
|
|
C. ‘Psychogenic’ events |
Hypoventilation 3 |
3
|
|
C. ‘Psychogenic’ events |
Nausea 3 |
3
|
|
C. ‘Psychogenic’ events |
Pain 3 |
3
|
|
C. ‘Psychogenic’ events |
Pain in extremity 3 |
3
|
|
C. ‘Psychogenic’ events |
Panic reaction 3 |
3
|
|
C. ‘Psychogenic’ events |
Rash 3 |
3
|
|
C. ‘Psychogenic’ events |
Sensory loss 3 |
3
|
|
C. ‘Psychogenic’ events |
Somnolence 3 |
3
|
|
C. ‘Psychogenic’ events |
Throat irritation 3 |
3
|
|
C. ‘Psychogenic’ events |
Vertigo 3 |
3
|
|
C. ‘Psychogenic’ events |
Amnesia 2 |
2
|
|
C. ‘Psychogenic’ events |
Blood pressure increased 2 |
2
|
|
C. ‘Psychogenic’ events |
Body temperature decreased 2 |
2
|
|
C. ‘Psychogenic’ events |
Bradycardia 2 |
2
|
|
C. ‘Psychogenic’ events |
Circulatory collapse 2 |
2
|
|
C. ‘Psychogenic’ events |
Colour blindness acquired 2 |
2
|
|
C. ‘Psychogenic’ events |
Consciousness fluctuating 2 |
2
|
|
C. ‘Psychogenic’ events |
Diplopia 2 |
2
|
|
C. ‘Psychogenic’ events |
Dry mouth 2 |
2
|
|
C. ‘Psychogenic’ events |
Dry throat 2 |
2
|
|
C. ‘Psychogenic’ events |
Dysarthria 2 |
2
|
|
C. ‘Psychogenic’ events |
Dysphagia 2 |
2
|
|
C. ‘Psychogenic’ events |
Emotional distress 2 |
2
|
|
C. ‘Psychogenic’ events |
Heart rate decreased 2 |
2
|
|
C. ‘Psychogenic’ events |
Heart rate increased 2 |
2
|
|
C. ‘Psychogenic’ events |
Hypertension 2 |
2
|
|
C. ‘Psychogenic’ events |
Hyperventilation 2 |
2
|
|
C. ‘Psychogenic’ events |
Hypoacusis 2 |
2
|
|
C. ‘Psychogenic’ events |
Malaise 2 |
2
|
|
C. ‘Psychogenic’ events |
Muscular weakness 2 |
2
|
|
C. ‘Psychogenic’ events |
Myalgia 2 |
2
|
|
C. ‘Psychogenic’ events |
Neck pain 2 |
2
|
|
C. ‘Psychogenic’ events |
Oropharyngeal pain 2 |
2
|
|
C. ‘Psychogenic’ events |
Paraesthesia oral 2 |
2
|
|
C. ‘Psychogenic’ events |
Presyncope 2 |
2
|
|
C. ‘Psychogenic’ events |
Procedural dizziness 2 |
2
|
|
C. ‘Psychogenic’ events |
Pruritus 2 |
2
|
|
C. ‘Psychogenic’ events |
Pulse pressure decreased 2 |
2
|
|
C. ‘Psychogenic’ events |
Pupil fixed 2 |
2
|
|
C. ‘Psychogenic’ events |
Rash generalised 2 |
2
|
|
C. ‘Psychogenic’ events |
Retching 2 |
2
|
|
C. ‘Psychogenic’ events |
Salivary hypersecretion 2 |
2
|
|
C. ‘Psychogenic’ events |
Shock 2 |
2
|
|
C. ‘Psychogenic’ events |
Vision blurred 2 |
2
|
|
C. ‘Psychogenic’ events |
Abdominal discomfort 1 |
1
|
|
C. ‘Psychogenic’ events |
Abdominal distension 1 |
1
|
|
C. ‘Psychogenic’ events |
Abdominal pain 1 |
1
|
|
C. ‘Psychogenic’ events |
Abnormal behaviour 1 |
1
|
|
C. ‘Psychogenic’ events |
Altered state of consciousness 1 |
1
|
|
C. ‘Psychogenic’ events |
Aphasia 1 |
1
|
|
C. ‘Psychogenic’ events |
Asthenia 1 |
1
|
|
C. ‘Psychogenic’ events |
Asthma 1 |
1
|
|
C. ‘Psychogenic’ events |
Back pain 1 |
1
|
|
C. ‘Psychogenic’ events |
Blindness transient 1 |
1
|
|
C. ‘Psychogenic’ events |
Blood pressure increased 1 |
1
|
|
C. ‘Psychogenic’ events |
Blood pressure systolic decreased 1 |
1
|
|
C. ‘Psychogenic’ events |
Body temperature decreased 1 |
1
|
|
C. ‘Psychogenic’ events |
Bruxism 1 |
1
|
|
C. ‘Psychogenic’ events |
Burning sensation 1 |
1
|
|
C. ‘Psychogenic’ events |
Chills 1 |
1
|
|
C. ‘Psychogenic’ events |
Condition aggravated 1 |
1
|
|
C. ‘Psychogenic’ events |
Convulsion 1 |
1
|
|
C. ‘Psychogenic’ events |
Cough 1 |
1
|
|
C. ‘Psychogenic’ events |
Deafness transitory 1 |
1
|
|
C. ‘Psychogenic’ events |
Depressed level of consciousness 1 |
1
|
|
C. ‘Psychogenic’ events |
Discomfort 1 |
1
|
|
C. ‘Psychogenic’ events |
Dissociation 1 |
1
|
|
C. ‘Psychogenic’ events |
Disturbance in attention 1 |
1
|
|
C. ‘Psychogenic’ events |
Dry mouth 1 |
1
|
|
C. ‘Psychogenic’ events |
Ear discomfort 1 |
1
|
|
C. ‘Psychogenic’ events |
Ear pain 1 |
1
|
|
C. ‘Psychogenic’ events |
Epistaxis 1 |
1
|
|
C. ‘Psychogenic’ events |
Eye pain 1 |
1
|
|
C. ‘Psychogenic’ events |
Eyelid oedema 1 |
1
|
|
C. ‘Psychogenic’ events |
Face injury 1 |
1
|
|
C. ‘Psychogenic’ events |
Facial spasm 1 |
1
|
|
C. ‘Psychogenic’ events |
Fatigue 1 |
1
|
|
C. ‘Psychogenic’ events |
Fear 1 |
1
|
|
C. ‘Psychogenic’ events |
Feeling of despair 1 |
1
|
|
C. ‘Psychogenic’ events |
Foaming at mouth 1 |
1
|
|
C. ‘Psychogenic’ events |
Gait disturbance 1 |
1
|
|
C. ‘Psychogenic’ events |
Grand mal convulsion 1 |
1
|
|
C. ‘Psychogenic’ events |
Grip strength decreased 1 |
1
|
|
C. ‘Psychogenic’ events |
Head banging 1 |
1
|
|
C. ‘Psychogenic’ events |
Head discomfort 1 |
1
|
|
C. ‘Psychogenic’ events |
Heart rate irregular 1 |
1
|
|
C. ‘Psychogenic’ events |
Heat rash 1 |
1
|
|
C. ‘Psychogenic’ events |
Hemiparesis 1 |
1
|
|
C. ‘Psychogenic’ events |
Hot flush 1 |
1
|
|
C. ‘Psychogenic’ events |
Hyperhidrosis 1 |
1
|
|
C. ‘Psychogenic’ events |
Hypersomnia 1 |
1
|
|
C. ‘Psychogenic’ events |
Hypoaesthesia 1 |
1
|
|
C. ‘Psychogenic’ events |
Hypoaesthesia facial 1 |
1
|
|
C. ‘Psychogenic’ events |
Hypokinesia 1 |
1
|
|
C. ‘Psychogenic’ events |
Hypotonia 1 |
1
|
|
C. ‘Psychogenic’ events |
Incontinence 1 |
1
|
|
C. ‘Psychogenic’ events |
Lip swelling 1 |
1
|
|
C. ‘Psychogenic’ events |
Livedo reticularis 1 |
1
|
|
C. ‘Psychogenic’ events |
Migraine 1 |
1
|
|
C. ‘Psychogenic’ events |
Muscle contracture 1 |
1
|
|
C. ‘Psychogenic’ events |
Myoclonus 1 |
1
|
|
C. ‘Psychogenic’ events |
Nervous system disorder 1 |
1
|
|
C. ‘Psychogenic’ events |
Oral discomfort 1 |
1
|
|
C. ‘Psychogenic’ events |
Palpitations 1 |
1
|
|
C. ‘Psychogenic’ events |
Paraesthesia 1 |
1
|
|
C. ‘Psychogenic’ events |
Peripheral circulatory failure 1 |
1
|
|
C. ‘Psychogenic’ events |
Pharyngeal oedema 1 |
1
|
|
C. ‘Psychogenic’ events |
Photophobia 1 |
1
|
|
C. ‘Psychogenic’ events |
Poor peripheral circulation 1 |
1
|
|
C. ‘Psychogenic’ events |
Pruritus 1 |
1
|
|
C. ‘Psychogenic’ events |
Psychomotor hyperactivity 1 |
1
|
|
C. ‘Psychogenic’ events |
Pyrexia 1 |
1
|
|
C. ‘Psychogenic’ events |
Respiratory arrest 1 |
1
|
|
C. ‘Psychogenic’ events |
Respiratory rate decreased 1 |
1
|
|
C. ‘Psychogenic’ events |
Seizure anoxic 1 |
1
|
|
C. ‘Psychogenic’ events |
Sensation of heaviness 1 |
1
|
|
C. ‘Psychogenic’ events |
Sensory loss 1 |
1
|
|
C. ‘Psychogenic’ events |
Sinus tachycardia 1 |
1
|
|
C. ‘Psychogenic’ events |
Sleep attacks 1 |
1
|
|
C. ‘Psychogenic’ events |
Sudden onset of sleep 1 |
1
|
|
C. ‘Psychogenic’ events |
Tachypnoea 1 |
1
|
|
C. ‘Psychogenic’ events |
Tremor 1 |
1
|
|
C. ‘Psychogenic’ events |
Urticaria 1 |
1
|
|
C. ‘Psychogenic’ events |
Visual impairment 1 |
1
|
|
D. ‘Other recognised’ reactions |
Nausea 631 |
631
|
|
D. ‘Other recognised’ reactions |
Headache 629 |
629
|
|
D. ‘Other recognised’ reactions |
Dizziness 625 |
625
|
|
D. ‘Other recognised’ reactions |
Vomiting 260 |
260
|
|
D. ‘Other recognised’ reactions |
Malaise 220 |
220
|
|
D. ‘Other recognised’ reactions |
Fatigue 216 |
216
|
|
D. ‘Other recognised’ reactions |
Pyrexia 175 |
175
|
|
D. ‘Other recognised’ reactions |
Abdominal pain 69 |
69
|
|
D. ‘Other recognised’ reactions |
Diarrhoea 55 |
55
|
|
D. ‘Other recognised’ reactions |
Abdominal pain upper 54 |
54
|
|
D. ‘Other recognised’ reactions |
Myalgia 49 |
49
|
|
D. ‘Other recognised’ reactions |
Lethargy 48 |
48
|
|
D. ‘Other recognised’ reactions |
Feeling hot 43 |
43
|
|
D. ‘Other recognised’ reactions |
Body temperature increased 36 |
36
|
|
D. ‘Other recognised’ reactions |
Pain 34 |
34
|
|
D. ‘Other recognised’ reactions |
Headache 30 |
30
|
|
D. ‘Other recognised’ reactions |
Influenza like illness 28 |
28
|
|
D. ‘Other recognised’ reactions |
Nausea 28 |
28
|
|
D. ‘Other recognised’ reactions |
Oropharyngeal pain 28 |
28
|
|
D. ‘Other recognised’ reactions |
Arthralgia 25 |
25
|
|
D. ‘Other recognised’ reactions |
Malaise 25 |
25
|
|
D. ‘Other recognised’ reactions |
Pyrexia 24 |
24
|
|
D. ‘Other recognised’ reactions |
Pallor 22 |
22
|
|
D. ‘Other recognised’ reactions |
Somnolence 22 |
22
|
|
D. ‘Other recognised’ reactions |
Asthenia 21 |
21
|
|
D. ‘Other recognised’ reactions |
Chills 21 |
21
|
|
D. ‘Other recognised’ reactions |
Pain in extremity 21 |
21
|
|
D. ‘Other recognised’ reactions |
Rash 21 |
21
|
| Musculoskeletal and connective tissue disorders |
D. ‘Other recognised’ reactions |
Arthralgia 20 |
20
|
|
D. ‘Other recognised’ reactions |
Lymphadenopathy 18 |
18
|
|
D. ‘Other recognised’ reactions |
Vomiting 16 |
16
|
|
D. ‘Other recognised’ reactions |
Abdominal discomfort 15 |
15
|
|
D. ‘Other recognised’ reactions |
Dizziness 15 |
15
|
|
D. ‘Other recognised’ reactions |
Flushing 14 |
14
|
|
D. ‘Other recognised’ reactions |
Paraesthesia 14 |
14
|
|
D. ‘Other recognised’ reactions |
Fatigue 12 |
12
|
|
D. ‘Other recognised’ reactions |
Tremor 12 |
12
|
|
D. ‘Other recognised’ reactions |
Pruritus 11 |
11
|
|
D. ‘Other recognised’ reactions |
Decreased appetite 10 |
10
|
|
D. ‘Other recognised’ reactions |
Abdominal pain 8 |
8
|
|
D. ‘Other recognised’ reactions |
Neck pain 8 |
8
|
|
D. ‘Other recognised’ reactions |
Feeling cold 7 |
7
|
|
D. ‘Other recognised’ reactions |
Back pain 6 |
6
|
|
D. ‘Other recognised’ reactions |
Cough 6 |
6
|
|
D. ‘Other recognised’ reactions |
Hyperhidrosis 6 |
6
|
|
D. ‘Other recognised’ reactions |
Hypoaesthesia 6 |
6
|
|
D. ‘Other recognised’ reactions |
Lethargy 6 |
6
|
|
D. ‘Other recognised’ reactions |
Musculoskeletal stiffness 6 |
6
|
|
D. ‘Other recognised’ reactions |
Nasopharyngitis 6 |
6
|
|
D. ‘Other recognised’ reactions |
Abdominal pain upper 5 |
5
|
|
D. ‘Other recognised’ reactions |
Asthenia 4 |
4
|
|
D. ‘Other recognised’ reactions |
Body temperature increased 4 |
4
|
|
D. ‘Other recognised’ reactions |
Erythema 4 |
4
|
|
D. ‘Other recognised’ reactions |
Feeling of body temperature change 4 |
4
|
|
D. ‘Other recognised’ reactions |
Migraine 4 |
4
|
|
D. ‘Other recognised’ reactions |
Myalgia 4 |
4
|
|
D. ‘Other recognised’ reactions |
Nervousness 4 |
4
|
|
D. ‘Other recognised’ reactions |
Back pain 3 |
3
|
|
D. ‘Other recognised’ reactions |
Decreased appetite 3 |
3
|
|
D. ‘Other recognised’ reactions |
Diarrhoea 3 |
3
|
|
D. ‘Other recognised’ reactions |
Lower respiratory tract infection 3 |
3
|
|
D. ‘Other recognised’ reactions |
Muscle fatigue 3 |
3
|
|
D. ‘Other recognised’ reactions |
Muscular weakness 3 |
3
|
|
D. ‘Other recognised’ reactions |
Rash generalised 3 |
3
|
|
D. ‘Other recognised’ reactions |
Somnolence 3 |
3
|
|
D. ‘Other recognised’ reactions |
Cold sweat 2 |
2
|
|
D. ‘Other recognised’ reactions |
Dizziness postural 2 |
2
|
|
D. ‘Other recognised’ reactions |
Feeling abnormal 2 |
2
|
|
D. ‘Other recognised’ reactions |
Gait disturbance 2 |
2
|
|
D. ‘Other recognised’ reactions |
Head discomfort 2 |
2
|
|
D. ‘Other recognised’ reactions |
Hot flush 2 |
2
|
|
D. ‘Other recognised’ reactions |
Influenza like illness 2 |
2
|
|
D. ‘Other recognised’ reactions |
Joint swelling 2 |
2
|
|
D. ‘Other recognised’ reactions |
Limb discomfort 2 |
2
|
|
D. ‘Other recognised’ reactions |
Listless 2 |
2
|
|
D. ‘Other recognised’ reactions |
Local reaction 2 |
2
|
|
D. ‘Other recognised’ reactions |
Musculoskeletal stiffness 2 |
2
|
|
D. ‘Other recognised’ reactions |
Nasal congestion 2 |
2
|
|
D. ‘Other recognised’ reactions |
Oropharyngeal pain 2 |
2
|
|
D. ‘Other recognised’ reactions |
Pain 2 |
2
|
|
D. ‘Other recognised’ reactions |
Pruritus generalised 2 |
2
|
|
D. ‘Other recognised’ reactions |
Rash macular 2 |
2
|
|
D. ‘Other recognised’ reactions |
Skin warm 2 |
2
|
|
D. ‘Other recognised’ reactions |
Throat irritation 2 |
2
|
|
D. ‘Other recognised’ reactions |
Abdominal pain lower 1 |
1
|
|
D. ‘Other recognised’ reactions |
Abdominal pain lower 1 |
1
|
|
D. ‘Other recognised’ reactions |
Arthralgia 1 |
1
|
|
D. ‘Other recognised’ reactions |
Axillary mass 1 |
1
|
|
D. ‘Other recognised’ reactions |
Bedridden 1 |
1
|
|
D. ‘Other recognised’ reactions |
Body temperature 1 |
1
|
|
D. ‘Other recognised’ reactions |
Body temperature fluctuation 1 |
1
|
|
D. ‘Other recognised’ reactions |
Body temperature fluctuation 1 |
1
|
|
D. ‘Other recognised’ reactions |
Cough 1 |
1
|
|
D. ‘Other recognised’ reactions |
Dyspnoea 1 |
1
|
|
D. ‘Other recognised’ reactions |
Feeling of body temperature change 1 |
1
|
|
D. ‘Other recognised’ reactions |
Gastrointestinal disorder 1 |
1
|
|
D. ‘Other recognised’ reactions |
Generalised erythema 1 |
1
|
|
D. ‘Other recognised’ reactions |
Groin pain 1 |
1
|
|
D. ‘Other recognised’ reactions |
Hot flush 1 |
1
|
|
D. ‘Other recognised’ reactions |
Hypoaesthesia 1 |
1
|
|
D. ‘Other recognised’ reactions |
Hypotension 1 |
1
|
|
D. ‘Other recognised’ reactions |
Ill-defined disorder 1 |
1
|
|
D. ‘Other recognised’ reactions |
Immunisation reaction 1 |
1
|
|
D. ‘Other recognised’ reactions |
Induration 1 |
1
|
|
D. ‘Other recognised’ reactions |
Insomnia 1 |
1
|
|
D. ‘Other recognised’ reactions |
Limb discomfort 1 |
1
|
|
D. ‘Other recognised’ reactions |
Local reaction 1 |
1
|
|
D. ‘Other recognised’ reactions |
Local swelling 1 |
1
|
|
D. ‘Other recognised’ reactions |
Loss of consciousness 1 |
1
|
|
D. ‘Other recognised’ reactions |
Lymphadenopathy 1 |
1
|
|
D. ‘Other recognised’ reactions |
Mobility decreased 1 |
1
|
|
D. ‘Other recognised’ reactions |
Muscle spasms 1 |
1
|
|
D. ‘Other recognised’ reactions |
Muscle twitching 1 |
1
|
|
D. ‘Other recognised’ reactions |
Musculoskeletal chest pain 1 |
1
|
|
D. ‘Other recognised’ reactions |
Musculoskeletal discomfort 1 |
1
|
|
D. ‘Other recognised’ reactions |
Musculoskeletal discomfort 1 |
1
|
|
D. ‘Other recognised’ reactions |
Musculoskeletal pain 1 |
1
|
|
D. ‘Other recognised’ reactions |
Neck pain 1 |
1
|
|
D. ‘Other recognised’ reactions |
Night sweats 1 |
1
|
|
D. ‘Other recognised’ reactions |
Pain in extremity 1 |
1
|
|
D. ‘Other recognised’ reactions |
Peripheral coldness 1 |
1
|
|
D. ‘Other recognised’ reactions |
Pharyngitis 1 |
1
|
|
D. ‘Other recognised’ reactions |
Rash erythematous 1 |
1
|
|
D. ‘Other recognised’ reactions |
Respiratory disorder 1 |
1
|
|
D. ‘Other recognised’ reactions |
Respiratory tract infection 1 |
1
|
|
D. ‘Other recognised’ reactions |
Restlessness 1 |
1
|
|
D. ‘Other recognised’ reactions |
Rhinorrhoea 1 |
1
|
|
D. ‘Other recognised’ reactions |
Sensation of heaviness 1 |
1
|
|
D. ‘Other recognised’ reactions |
Sudden onset of sleep 1 |
1
|
|
D. ‘Other recognised’ reactions |
Swelling 1 |
1
|
|
D. ‘Other recognised’ reactions |
Swelling face 1 |
1
|
|
D. ‘Other recognised’ reactions |
Syncope 1 |
1
|
|
D. ‘Other recognised’ reactions |
Thirst 1 |
1
|
|
D. ‘Other recognised’ reactions |
Throat tightness 1 |
1
|
|
D. ‘Other recognised’ reactions |
Upper respiratory tract infection 1 |
1
|
|
D. ‘Other recognised’ reactions |
Urticaria 1 |
1
|
|
D. ‘Other recognised’ reactions |
Weight decreased 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Headache 47 |
47
|
| Nervous system disorders |
E. not currently recognised |
Syncope 35 |
35
|
| General disorders and administration site conditions |
E. not currently recognised |
Influenza like illness 32 |
32
|
| Nervous system disorders |
E. not currently recognised |
Dizziness 29 |
29
|
| Nervous system disorders |
E. not currently recognised |
Hypoaesthesia 29 |
29
|
| Nervous system disorders |
E. not currently recognised |
Convulsion 28 |
28
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Pain in extremity 27 |
27
|
| Gastrointestinal disorders |
E. not currently recognised |
Nausea 24 |
24
|
| Nervous system disorders |
E. not currently recognised |
Paraesthesia 20 |
20
|
| Respiratory, thoracic and mediastinal disorders |
E. not currently recognised |
Dyspnoea 19 |
19
|
| Nervous system disorders |
E. not currently recognised |
Lethargy 19 |
19
|
| General disorders and administration site conditions |
E. not currently recognised |
Malaise 19 |
19
|
| Injury, poisoning and procedural complications |
E. not currently recognised |
Drug exposure during pregnancy 18 |
18
|
| General disorders and administration site conditions |
E. not currently recognised |
Fatigue 18 |
18
|
| General disorders and administration site conditions |
E. not currently recognised |
Pyrexia 18 |
18
|
| General disorders and administration site conditions |
E. not currently recognised |
Chest pain 17 |
17
|
| Gastrointestinal disorders |
E. not currently recognised |
Vomiting 17 |
17
|
| Nervous system disorders |
E. not currently recognised |
Migraine 16 |
16
|
| General disorders and administration site conditions |
E. not currently recognised |
Pain 16 |
16
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Back pain 15 |
15
|
| Nervous system disorders |
E. not currently recognised |
Somnolence 14 |
14
|
| Nervous system disorders |
E. not currently recognised |
Tremor 14 |
14
|
| Nervous system disorders |
E. not currently recognised |
Dizziness 12 |
12
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Muscular weakness 12 |
12
|
| Pregnancy, puerperium and perinatal conditions |
E. not currently recognised |
Abortion spontaneous 11 |
11
|
| General disorders and administration site conditions |
E. not currently recognised |
Asthenia 11 |
11
|
| Nervous system disorders |
E. not currently recognised |
Headache 11 |
11
|
| Nervous system disorders |
E. not currently recognised |
Loss of consciousness 11 |
11
|
| Gastrointestinal disorders |
E. not currently recognised |
Abdominal pain 10 |
10
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Myalgia 10 |
10
|
| Respiratory, thoracic and mediastinal disorders |
E. not currently recognised |
Oropharyngeal pain 10 |
10
|
| Reproductive system and breast disorders |
E. not currently recognised |
Amenorrhoea 9 |
9
|
| General disorders and administration site conditions |
E. not currently recognised |
Chest discomfort 9 |
9
|
| Vascular disorders |
E. not currently recognised |
Peripheral coldness 9 |
9
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Alopecia 8 |
8
|
| Respiratory, thoracic and mediastinal disorders |
E. not currently recognised |
Cough 8 |
8
|
| Metabolism and nutrition disorders |
E. not currently recognised |
Decreased appetite 8 |
8
|
| Respiratory, thoracic and mediastinal disorders |
E. not currently recognised |
Epistaxis 8 |
8
|
| General disorders and administration site conditions |
E. not currently recognised |
Fatigue 8 |
8
|
| General disorders and administration site conditions |
E. not currently recognised |
Influenza like illness 8 |
8
|
| Eye disorders |
E. not currently recognised |
Vision blurred 8 |
8
|
| Respiratory, thoracic and mediastinal disorders |
E. not currently recognised |
Asthma 7 |
7
|
| Gastrointestinal disorders |
E. not currently recognised |
Diarrhoea 7 |
7
|
| General disorders and administration site conditions |
E. not currently recognised |
Feeling cold 7 |
7
|
| Nervous system disorders |
E. not currently recognised |
Hypoaesthesia 7 |
7
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Hypoaesthesia facial 7 |
7
|
| Eye disorders |
E. not currently recognised |
Photophobia 7 |
7
|
| Nervous system disorders |
E. not currently recognised |
Syncope 7 |
7
|
| Reproductive system and breast disorders |
E. not currently recognised |
Vaginal haemorrhage 7 |
7
|
| Infections and infestations |
E. not currently recognised |
Viral infection 7 |
7
|
| Eye disorders |
E. not currently recognised |
Vision blurred 7 |
7
|
| Gastrointestinal disorders |
E. not currently recognised |
Abdominal pain 6 |
6
|
| Nervous system disorders |
E. not currently recognised |
Dysarthria 6 |
6
|
| Ear and labyrinth disorders |
E. not currently recognised |
Ear pain 6 |
6
|
| Nervous system disorders |
E. not currently recognised |
Epilepsy 6 |
6
|
| Psychiatric disorders |
E. not currently recognised |
Hallucination 6 |
6
|
| Psychiatric disorders |
E. not currently recognised |
Insomnia 6 |
6
|
| Infections and infestations |
E. not currently recognised |
Lower respiratory tract infection 6 |
6
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Musculoskeletal stiffness 6 |
6
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Neck pain 6 |
6
|
| Cardiac disorders |
E. not currently recognised |
Palpitations 6 |
6
|
| Nervous system disorders |
E. not currently recognised |
Paraesthesia 6 |
6
|
| Infections and infestations |
E. not currently recognised |
Post viral fatigue syndrome 6 |
6
|
| Nervous system disorders |
E. not currently recognised |
Sensory disturbance 6 |
6
|
| Eye disorders |
E. not currently recognised |
Visual impairment 6 |
6
|
| General disorders and administration site conditions |
E. not currently recognised |
Abasia 5 |
5
|
| Nervous system disorders |
E. not currently recognised |
Dyskinesia 5 |
5
|
| Nervous system disorders |
E. not currently recognised |
Dysstasia 5 |
5
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Eczema 5 |
5
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Erythema multiforme 5 |
5
|
| Nervous system disorders |
E. not currently recognised |
Facial palsy 5 |
5
|
| Nervous system disorders |
E. not currently recognised |
Grand mal convulsion 5 |
5
|
| Reproductive system and breast disorders |
E. not currently recognised |
Menstruation irregular 5 |
5
|
| General disorders and administration site conditions |
E. not currently recognised |
Oedema peripheral 5 |
5
|
| Vascular disorders |
E. not currently recognised |
Pallor 5 |
5
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Sensation of heaviness 5 |
5
|
| Investigations |
E. not currently recognised |
Weight decreased 5 |
5
|
| Psychiatric disorders |
E. not currently recognised |
Anxiety 4 |
4
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Arthralgia 4 |
4
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Blister 4 |
4
|
| Investigations |
E. not currently recognised |
Blood glucose increased 4 |
4
|
| General disorders and administration site conditions |
E. not currently recognised |
Chills 4 |
4
|
| General disorders and administration site conditions |
E. not currently recognised |
Chronic fatigue syndrome 4 |
4
|
| General disorders and administration site conditions |
E. not currently recognised |
Condition aggravated 4 |
4
|
| Psychiatric disorders |
E. not currently recognised |
Confusional state 4 |
4
|
| Injury, poisoning and procedural complications |
E. not currently recognised |
Contusion 4 |
4
|
| Cardiac disorders |
E. not currently recognised |
Cyanosis 4 |
4
|
| Reproductive system and breast disorders |
E. not currently recognised |
Dysmenorrhoea 4 |
4
|
| Nervous system disorders |
E. not currently recognised |
Encephalitis 4 |
4
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Erythema 4 |
4
|
| General disorders and administration site conditions |
E. not currently recognised |
Feeling hot 4 |
4
|
| Nervous system disorders |
E. not currently recognised |
Guillain-barre syndrome 4 |
4
|
| Vascular disorders |
E. not currently recognised |
Hypotension 4 |
4
|
| Nervous system disorders |
E. not currently recognised |
Lethargy 4 |
4
|
| Reproductive system and breast disorders |
E. not currently recognised |
Menorrhagia 4 |
4
|
| Infections and infestations |
E. not currently recognised |
Nasopharyngitis 4 |
4
|
| Gastrointestinal disorders |
E. not currently recognised |
Nausea 4 |
4
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Rash 4 |
4
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Rash 4 |
4
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Skin discolouration 4 |
4
|
| Respiratory, thoracic and mediastinal disorders |
E. not currently recognised |
Wheezing 4 |
4
|
| Surgical and medical procedures |
E. not currently recognised |
Abortion induced 3 |
3
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Alopecia 3 |
3
|
| Nervous system disorders |
E. not currently recognised |
Aphonia 3 |
3
|
| Nervous system disorders |
E. not currently recognised |
Convulsion 3 |
3
|
| Psychiatric disorders |
E. not currently recognised |
Disorientation 3 |
3
|
| Ear and labyrinth disorders |
E. not currently recognised |
Ear pain 3 |
3
|
| Nervous system disorders |
E. not currently recognised |
Epilepsy 3 |
3
|
| General disorders and administration site conditions |
E. not currently recognised |
Feeling abnormal 3 |
3
|
| Nervous system disorders |
E. not currently recognised |
Head discomfort 3 |
3
|
| Nervous system disorders |
E. not currently recognised |
Hemiparesis 3 |
3
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Hyperhidrosis 3 |
3
|
| Infections and infestations |
E. not currently recognised |
Infectious mononucleosis 3 |
3
|
| Pregnancy, puerperium and perinatal conditions |
E. not currently recognised |
Live birth 3 |
3
|
| Reproductive system and breast disorders |
E. not currently recognised |
Menstruation delayed 3 |
3
|
| Gastrointestinal disorders |
E. not currently recognised |
Mouth ulceration 3 |
3
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Muscle twitching 3 |
3
|
| Eye disorders |
E. not currently recognised |
Mydriasis 3 |
3
|
| Vascular disorders |
E. not currently recognised |
Peripheral coldness 3 |
3
|
| Pregnancy, puerperium and perinatal conditions |
E. not currently recognised |
Premature baby 3 |
3
|
| General disorders and administration site conditions |
E. not currently recognised |
Pyrexia 3 |
3
|
| Nervous system disorders |
E. not currently recognised |
Sensory loss 3 |
3
|
| Psychiatric disorders |
E. not currently recognised |
Tearfulness 3 |
3
|
| Nervous system disorders |
E. not currently recognised |
Tremor 3 |
3
|
| Nervous system disorders |
E. not currently recognised |
Unresponsive to stimuli 3 |
3
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Urticaria 3 |
3
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Urticaria chronic 3 |
3
|
| Nervous system disorders |
E. not currently recognised |
Visual field defect 3 |
3
|
| General disorders and administration site conditions |
E. not currently recognised |
Abasia 2 |
2
|
| Gastrointestinal disorders |
E. not currently recognised |
Abdominal pain upper 2 |
2
|
| Psychiatric disorders |
E. not currently recognised |
Abnormal behaviour 2 |
2
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Alopecia areata 2 |
2
|
| Reproductive system and breast disorders |
E. not currently recognised |
Amenorrhoea 2 |
2
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Angioedema 2 |
2
|
| Nervous system disorders |
E. not currently recognised |
Balance disorder 2 |
2
|
| Investigations |
E. not currently recognised |
Body temperature increased 2 |
2
|
| Vascular disorders |
E. not currently recognised |
Circulatory collapse 2 |
2
|
| Nervous system disorders |
E. not currently recognised |
Complex regional pain syndrome 2 |
2
|
| Nervous system disorders |
E. not currently recognised |
Complex regional pain syndrome 2 |
2
|
| Psychiatric disorders |
E. not currently recognised |
Confusional state 2 |
2
|
| Nervous system disorders |
E. not currently recognised |
Crying 2 |
2
|
| Metabolism and nutrition disorders |
E. not currently recognised |
Dehydration 2 |
2
|
| Psychiatric disorders |
E. not currently recognised |
Depressed mood 2 |
2
|
| Nervous system disorders |
E. not currently recognised |
Diplegia 2 |
2
|
| Eye disorders |
E. not currently recognised |
Diplopia 2 |
2
|
| Nervous system disorders |
E. not currently recognised |
Disturbance in attention 2 |
2
|
| Nervous system disorders |
E. not currently recognised |
Dizziness postural 2 |
2
|
| Nervous system disorders |
E. not currently recognised |
Drooling 2 |
2
|
| Injury, poisoning and procedural complications |
E. not currently recognised |
Drug exposure before pregnancy 2 |
2
|
| Nervous system disorders |
E. not currently recognised |
Dysgeusia 2 |
2
|
| Psychiatric disorders |
E. not currently recognised |
Emotional disorder 2 |
2
|
| Eye disorders |
E. not currently recognised |
Eye pain 2 |
2
|
| Nervous system disorders |
E. not currently recognised |
Facial paresis 2 |
2
|
| General disorders and administration site conditions |
E. not currently recognised |
Feeling cold 2 |
2
|
| General disorders and administration site conditions |
E. not currently recognised |
Gait disturbance 2 |
2
|
| General disorders and administration site conditions |
E. not currently recognised |
Gait disturbance 2 |
2
|
| Nervous system disorders |
E. not currently recognised |
Grand mal convulsion 2 |
2
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Groin pain 2 |
2
|
| Respiratory, thoracic and mediastinal disorders |
E. not currently recognised |
Haemoptysis 2 |
2
|
| Vascular disorders |
E. not currently recognised |
Haemorrhage 2 |
2
|
| Infections and infestations |
E. not currently recognised |
Herpes zoster 2 |
2
|
| Infections and infestations |
E. not currently recognised |
Hordeolum 2 |
2
|
| Vascular disorders |
E. not currently recognised |
Hot flush 2 |
2
|
| Respiratory, thoracic and mediastinal disorders |
E. not currently recognised |
Hyperventilation 2 |
2
|
| Nervous system disorders |
E. not currently recognised |
Hypokinesia 2 |
2
|
| Infections and infestations |
E. not currently recognised |
Influenza 2 |
2
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Joint swelling 2 |
2
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Livedo reticularis 2 |
2
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Livedo reticularis 2 |
2
|
| General disorders and administration site conditions |
E. not currently recognised |
Local swelling 2 |
2
|
| Nervous system disorders |
E. not currently recognised |
Loss of consciousness 2 |
2
|
| General disorders and administration site conditions |
E. not currently recognised |
Malaise 2 |
2
|
| Reproductive system and breast disorders |
E. not currently recognised |
Menstrual disorder 2 |
2
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Mobility decreased 2 |
2
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Muscle spasms 2 |
2
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Muscular weakness 2 |
2
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Musculoskeletal pain 2 |
2
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Musculoskeletal stiffness 2 |
2
|
| Nervous system disorders |
E. not currently recognised |
Optic neuritis 2 |
2
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Pain in extremity 2 |
2
|
| Vascular disorders |
E. not currently recognised |
Pallor 2 |
2
|
| Gastrointestinal disorders |
E. not currently recognised |
Paraesthesia oral 2 |
2
|
| Nervous system disorders |
E. not currently recognised |
Petit mal epilepsy 2 |
2
|
| Infections and infestations |
E. not currently recognised |
Pharyngitis 2 |
2
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Photosensitivity reaction 2 |
2
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Photosensitivity reaction 2 |
2
|
| Congenital, familial and genetic disorders |
E. not currently recognised |
Pilonidal cyst congenital 2 |
2
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Purpura 2 |
2
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Rash generalised 2 |
2
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Rheumatoid arthritis 2 |
2
|
| Respiratory, thoracic and mediastinal disorders |
E. not currently recognised |
Rhinorrhoea 2 |
2
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Skin exfoliation 2 |
2
|
| Psychiatric disorders |
E. not currently recognised |
Sleep disorder 2 |
2
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Swelling face 2 |
2
|
| Cardiac disorders |
E. not currently recognised |
Tachycardia 2 |
2
|
| Renal and urinary disorders |
E. not currently recognised |
Urinary incontinence 2 |
2
|
| Renal and urinary disorders |
E. not currently recognised |
Urinary retention 2 |
2
|
| Infections and infestations |
E. not currently recognised |
Urinary tract infection 2 |
2
|
| Ear and labyrinth disorders |
E. not currently recognised |
Vertigo 2 |
2
|
| Eye disorders |
E. not currently recognised |
Visual impairment 2 |
2
|
| Reproductive system and breast disorders |
E. not currently recognised |
Vulval ulceration 2 |
2
|
| Investigations |
E. not currently recognised |
Weight increased 2 |
2
|
| Gastrointestinal disorders |
E. not currently recognised |
Abdominal discomfort 1 |
1
|
| Gastrointestinal disorders |
E. not currently recognised |
Abdominal discomfort 1 |
1
|
| Gastrointestinal disorders |
E. not currently recognised |
Abdominal pain lower 1 |
1
|
| Gastrointestinal disorders |
E. not currently recognised |
Abdominal pain upper 1 |
1
|
| Gastrointestinal disorders |
E. not currently recognised |
Abnormal faeces 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Abnormal sleep-related event 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Abscess 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Acarodermatitis 1 |
1
|
| Eye disorders |
E. not currently recognised |
Accommodation disorder 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Acne 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Acne 1 |
1
|
| Neoplasms benign, malignant and unspecified (incl cysts and polyps) |
E. not currently recognised |
Acute myeloid leukaemia 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Acute psychosis 1 |
1
|
| Respiratory, thoracic and mediastinal disorders |
E. not currently recognised |
Acute respiratory failure 1 |
1
|
| Endocrine disorders |
E. not currently recognised |
Adrenocortical insufficiency acute 1 |
1
|
| Endocrine disorders |
E. not currently recognised |
Adrenocortical insufficiency acute 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Aggression 1 |
1
|
| Investigations |
E. not currently recognised |
Alanine aminotransferase increased 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Alopecia areata 1 |
1
|
| Blood and lymphatic system disorders |
E. not currently recognised |
Anaemia 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Anogenital warts 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Aphasia 1 |
1
|
| Blood and lymphatic system disorders |
E. not currently recognised |
Aplastic anaemia 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Application site pustules 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Areflexia 1 |
1
|
| Congenital, familial and genetic disorders |
E. not currently recognised |
Arteriovenous malformation 1 |
1
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Arthritis 1 |
1
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Arthritis reactive 1 |
1
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Arthropathy 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Asthenia 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Ataxia 1 |
1
|
| Injury, poisoning and procedural complications |
E. not currently recognised |
Axillary nerve injury 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Axillary pain 1 |
1
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Back pain 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Balance disorder 1 |
1
|
| Neoplasms benign, malignant and unspecified (incl cysts and polyps) |
E. not currently recognised |
Benign hydatidiform mole 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Beta haemolytic streptococcal infection 1 |
1
|
| Eye disorders |
E. not currently recognised |
Blindness unilateral 1 |
1
|
| Investigations |
E. not currently recognised |
Blood cortisol decreased 1 |
1
|
| Investigations |
E. not currently recognised |
Blood pressure decreased 1 |
1
|
| Investigations |
E. not currently recognised |
Blood pressure increased 1 |
1
|
| Investigations |
E. not currently recognised |
Body temperature increased 1 |
1
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Bone pain 1 |
1
|
| Reproductive system and breast disorders |
E. not currently recognised |
Breast pain 1 |
1
|
| Reproductive system and breast disorders |
E. not currently recognised |
Breast swelling 1 |
1
|
| Reproductive system and breast disorders |
E. not currently recognised |
Breast tenderness 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Bronchitis 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Burning sensation 1 |
1
|
| Cardiac disorders |
E. not currently recognised |
Cardiac arrest 1 |
1
|
| Investigations |
E. not currently recognised |
Cell marker increased 1 |
1
|
| Congenital, familial and genetic disorders |
E. not currently recognised |
Cerebral palsy 1 |
1
|
| Reproductive system and breast disorders |
E. not currently recognised |
Cervix inflammation 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Chest discomfort 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Chest pain 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Chills 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Chorea 1 |
1
|
| Congenital, familial and genetic disorders |
E. not currently recognised |
Cleft palate 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Cold sweat 1 |
1
|
| Gastrointestinal disorders |
E. not currently recognised |
Colitis 1 |
1
|
| Gastrointestinal disorders |
E. not currently recognised |
Colitis ulcerative 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Condition aggravated 1 |
1
|
| Eye disorders |
E. not currently recognised |
Conjunctival hyperaemia 1 |
1
|
| Gastrointestinal disorders |
E. not currently recognised |
Constipation 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Coordination abnormal 1 |
1
|
| Investigations |
E. not currently recognised |
Csf cell count increased 1 |
1
|
| Eye disorders |
E. not currently recognised |
Dark circles under eyes 1 |
1
|
| Ear and labyrinth disorders |
E. not currently recognised |
Deafness 1 |
1
|
| Ear and labyrinth disorders |
E. not currently recognised |
Deafness bilateral 1 |
1
|
| Metabolism and nutrition disorders |
E. not currently recognised |
Decreased appetite 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Decreased interest 1 |
1
|
| Vascular disorders |
E. not currently recognised |
Deep vein thrombosis 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Depressed level of consciousness 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Depression 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Depression 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Depressive symptom 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Dermatitis allergic 1 |
1
|
| Metabolism and nutrition disorders |
E. not currently recognised |
Diabetes mellitus inadequate control 1 |
1
|
| Metabolism and nutrition disorders |
E. not currently recognised |
Diabetes mellitus inadequate control 1 |
1
|
| Metabolism and nutrition disorders |
E. not currently recognised |
Diabetic ketoacidosis 1 |
1
|
| Gastrointestinal disorders |
E. not currently recognised |
Diarrhoea 1 |
1
|
| Gastrointestinal disorders |
E. not currently recognised |
Diarrhoea haemorrhagic 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Discomfort 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Dissociation 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Dizziness postural 1 |
1
|
| Eye disorders |
E. not currently recognised |
Dry eye 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Dry skin 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Dysgeusia 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Dyskinesia 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Dysphemia 1 |
1
|
| Respiratory, thoracic and mediastinal disorders |
E. not currently recognised |
Dyspnoea 1 |
1
|
| Ear and labyrinth disorders |
E. not currently recognised |
Ear discomfort 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Eating disorder 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Eczema vesicular 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Emotional distress 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Encephalitis 1 |
1
|
| Blood and lymphatic system disorders |
E. not currently recognised |
Eosinophilia 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Erythema 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Erythema multiforme 1 |
1
|
| Eye disorders |
E. not currently recognised |
Excessive eye blinking 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Exercise tolerance decreased 1 |
1
|
| Eye disorders |
E. not currently recognised |
Eye discharge 1 |
1
|
| Eye disorders |
E. not currently recognised |
Eye disorder 1 |
1
|
| Eye disorders |
E. not currently recognised |
Eye pain 1 |
1
|
| Eye disorders |
E. not currently recognised |
Eye swelling 1 |
1
|
| Eye disorders |
E. not currently recognised |
Eyelid oedema 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Facial palsy 1 |
1
|
| Injury, poisoning and procedural complications |
E. not currently recognised |
Fall 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Fear 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Feeling abnormal 1 |
1
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Flank pain 1 |
1
|
| Gastrointestinal disorders |
E. not currently recognised |
Flatulence 1 |
1
|
| Vascular disorders |
E. not currently recognised |
Flushing 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Folliculitis 1 |
1
|
| Gastrointestinal disorders |
E. not currently recognised |
Frequent bowel movements 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Furuncle 1 |
1
|
| Gastrointestinal disorders |
E. not currently recognised |
Gastrointestinal disorder 1 |
1
|
| Eye disorders |
E. not currently recognised |
Gaze palsy 1 |
1
|
| Gastrointestinal disorders |
E. not currently recognised |
Gingival disorder 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Guillain-barre syndrome 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Guttate psoriasis 1 |
1
|
| Blood and lymphatic system disorders |
E. not currently recognised |
Haemolytic uraemic syndrome 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Hallucination, auditory 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Hallucination, visual 1 |
1
|
| Congenital, familial and genetic disorders |
E. not currently recognised |
Heart disease congenital 1 |
1
|
| Investigations |
E. not currently recognised |
Heart rate decreased 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Henoch-schonlein purpura 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Henoch-schonlein purpura 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Hepatitis viral 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Herpes zoster 1 |
1
|
| Ear and labyrinth disorders |
E. not currently recognised |
Hyperacusis 1 |
1
|
| Metabolism and nutrition disorders |
E. not currently recognised |
Hyperglycaemia 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Hyperhidrosis 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Hyperpyrexia 1 |
1
|
| Immune system disorders |
E. not currently recognised |
Hypersensitivity 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Hypertonia 1 |
1
|
| Ear and labyrinth disorders |
E. not currently recognised |
Hypoacusis 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Hypoaesthesia facial 1 |
1
|
| Gastrointestinal disorders |
E. not currently recognised |
Hypoaesthesia oral 1 |
1
|
| Metabolism and nutrition disorders |
E. not currently recognised |
Hypoglycaemia 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Hypomania 1 |
1
|
| Congenital, familial and genetic disorders |
E. not currently recognised |
Hypospadias 1 |
1
|
| Respiratory, thoracic and mediastinal disorders |
E. not currently recognised |
Hypoventilation 1 |
1
|
| Injury, poisoning and procedural complications |
E. not currently recognised |
Inappropriate schedule of drug administration 1 |
1
|
| Injury, poisoning and procedural complications |
E. not currently recognised |
Incorrect dose administered 1 |
1
|
| Metabolism and nutrition disorders |
E. not currently recognised |
Increased appetite 1 |
1
|
| Respiratory, thoracic and mediastinal disorders |
E. not currently recognised |
Increased upper airway secretion 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Infection 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Inflammation 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Injection site erythema 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Injection site injury 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Injection site swelling 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Insomnia 1 |
1
|
| Gastrointestinal disorders |
E. not currently recognised |
Intestinal functional disorder 1 |
1
|
| Gastrointestinal disorders |
E. not currently recognised |
Irritable bowel syndrome 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Ivth nerve paralysis 1 |
1
|
| Hepatobiliary disorders |
E. not currently recognised |
Jaundice 1 |
1
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Joint stiffness 1 |
1
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Joint stiffness 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Kidney infection 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Labyrinthitis 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Laryngitis 1 |
1
|
| Congenital, familial and genetic disorders |
E. not currently recognised |
Limb malformation 1 |
1
|
| Gastrointestinal disorders |
E. not currently recognised |
Lip blister 1 |
1
|
| Gastrointestinal disorders |
E. not currently recognised |
Lip swelling 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Local swelling 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Meningism 1 |
1
|
| Reproductive system and breast disorders |
E. not currently recognised |
Menorrhagia 1 |
1
|
| Reproductive system and breast disorders |
E. not currently recognised |
Menstrual disorder 1 |
1
|
| Reproductive system and breast disorders |
E. not currently recognised |
Menstruation delayed 1 |
1
|
| Reproductive system and breast disorders |
E. not currently recognised |
Menstruation irregular 1 |
1
|
| Reproductive system and breast disorders |
E. not currently recognised |
Metrorrhagia 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Migraine 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Migraine with aura 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Molluscum contagiosum 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Monoplegia 1 |
1
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Muscle rigidity 1 |
1
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Muscle twitching 1 |
1
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Musculoskeletal chest pain 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Myoclonic epilepsy 1 |
1
|
| Respiratory, thoracic and mediastinal disorders |
E. not currently recognised |
Nasal congestion 1 |
1
|
| Neoplasms benign, malignant and unspecified (incl cysts and polyps) |
E. not currently recognised |
Neoplasm malignant 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Neuritis 1 |
1
|
| Renal and urinary disorders |
E. not currently recognised |
Neurogenic bladder 1 |
1
|
| Blood and lymphatic system disorders |
E. not currently recognised |
Neutropenia 1 |
1
|
| Investigations |
E. not currently recognised |
Neutrophil count decreased 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Oedema peripheral 1 |
1
|
| Respiratory, thoracic and mediastinal disorders |
E. not currently recognised |
Oropharyngeal blistering 1 |
1
|
| Respiratory, thoracic and mediastinal disorders |
E. not currently recognised |
Oropharyngeal pain 1 |
1
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Osteitis 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Otitis media 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Pain 1 |
1
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Palindromic rheumatism 1 |
1
|
| Blood and lymphatic system disorders |
E. not currently recognised |
Pancytopenia 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Paralysis 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Paranoia 1 |
1
|
| Investigations |
E. not currently recognised |
Peak expiratory flow rate decreased 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Petechiae 1 |
1
|
| Eye disorders |
E. not currently recognised |
Photopsia 1 |
1
|
| Investigations |
E. not currently recognised |
Platelet count decreased 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Pneumonia viral 1 |
1
|
| Renal and urinary disorders |
E. not currently recognised |
Pollakiuria 1 |
1
|
| Pregnancy, puerperium and perinatal conditions |
E. not currently recognised |
Pregnancy with injectable contraceptive 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Presyncope 1 |
1
|
| Respiratory, thoracic and mediastinal disorders |
E. not currently recognised |
Productive cough 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Psoriasis 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Psychiatric symptom 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Psychomotor hyperactivity 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Psychotic disorder 1 |
1
|
| Investigations |
E. not currently recognised |
Radial pulse 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Radiculitis brachial 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Rash erythematous 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Rash maculo-papular 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Rash vesicular 1 |
1
|
| Renal and urinary disorders |
E. not currently recognised |
Renal failure 1 |
1
|
| Investigations |
E. not currently recognised |
Respiratory rate increased 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Respiratory syncytial virus infection 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Respiratory tract infection 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Screaming 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Sedation 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Sensation of foreign body 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Sensation of pressure 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Sensory loss 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Sepsis 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Severe acute respiratory syndrome 1 |
1
|
| Cardiac disorders |
E. not currently recognised |
Sinus tachycardia 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Skin burning sensation 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Skin disorder 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Skin hypertrophy 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Skin infection 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Skin irritation 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Skin lesion 1 |
1
|
| Psychiatric disorders |
E. not currently recognised |
Somatisation disorder 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Somnolence 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Speech disorder 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Staphylococcal infection 1 |
1
|
| Nervous system disorders |
E. not currently recognised |
Status epilepticus 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Streptococcal sepsis 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Swelling 1 |
1
|
| Gastrointestinal disorders |
E. not currently recognised |
Swollen tongue 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Systemic inflammatory response syndrome 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Temperature intolerance 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Tenderness 1 |
1
|
| General disorders and administration site conditions |
E. not currently recognised |
Thirst 1 |
1
|
| Respiratory, thoracic and mediastinal disorders |
E. not currently recognised |
Throat tightness 1 |
1
|
| Ear and labyrinth disorders |
E. not currently recognised |
Tinnitus 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Trichorrhexis 1 |
1
|
| Metabolism and nutrition disorders |
E. not currently recognised |
Type 1 diabetes mellitus 1 |
1
|
| Respiratory, thoracic and mediastinal disorders |
E. not currently recognised |
Upper airway obstruction 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Upper respiratory tract infection 1 |
1
|
| Renal and urinary disorders |
E. not currently recognised |
Urinary retention 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Urticaria 1 |
1
|
| Reproductive system and breast disorders |
E. not currently recognised |
Vaginal discharge 1 |
1
|
| Reproductive system and breast disorders |
E. not currently recognised |
Vaginal lesion 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Varicella 1 |
1
|
| Infections and infestations |
E. not currently recognised |
Viraemia 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Vitiligo 1 |
1
|
| Eye disorders |
E. not currently recognised |
Vitreous floaters 1 |
1
|
| Gastrointestinal disorders |
E. not currently recognised |
Vomiting 1 |
1
|
| Musculoskeletal and connective tissue disorders |
E. not currently recognised |
Weight bearing difficulty 1 |
1
|
| Investigations |
E. not currently recognised |
Weight decreased 1 |
1
|
| Respiratory, thoracic and mediastinal disorders |
E. not currently recognised |
Wheezing 1 |
1
|
| Injury, poisoning and procedural complications |
E. not currently recognised |
Wrong technique in drug usage process 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Yellow skin 1 |
1
|
| Skin and subcutaneous tissue disorders |
E. not currently recognised |
Stevens-johnson syndrome 1 |
|


#9 by sTeamTraen » Fri Jan 03, 2014 10:46 pm











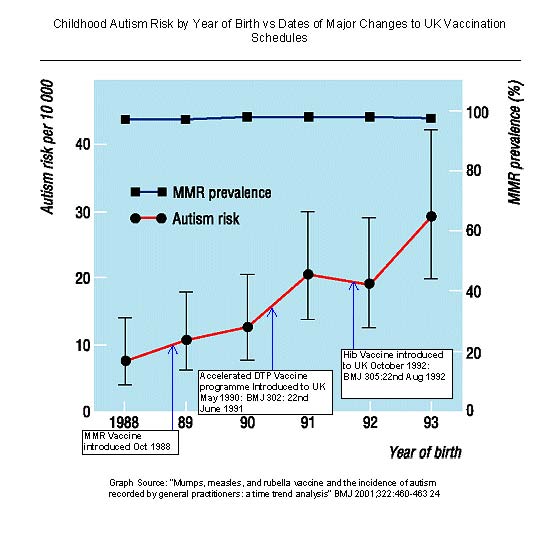








You must be logged in to post a comment.